fetching data ... 
Background: Measurement of intima-media thickness (IMT) has gained interest in the ultrasound (US) diagnostic of giant cell arteritis (GCA) but is not yet established in clinical routine.
Objectives: To evaluate the diagnostic accuracy of quantitative IMT measurement by US for diagnosing GCA.
Methods: A systematic literature review of the following electronic databases was performed: PubMed, Embase, Web of Science, Scopus, Lilacs, and Google Scholar (no date and language restriction, last search June 3, 2024). Studies that tested IMT`s diagnostic accuracy as a primary outcome in GCA suspected patients were included. The quality of the studies was assessed using the QUADAS-2 tool.
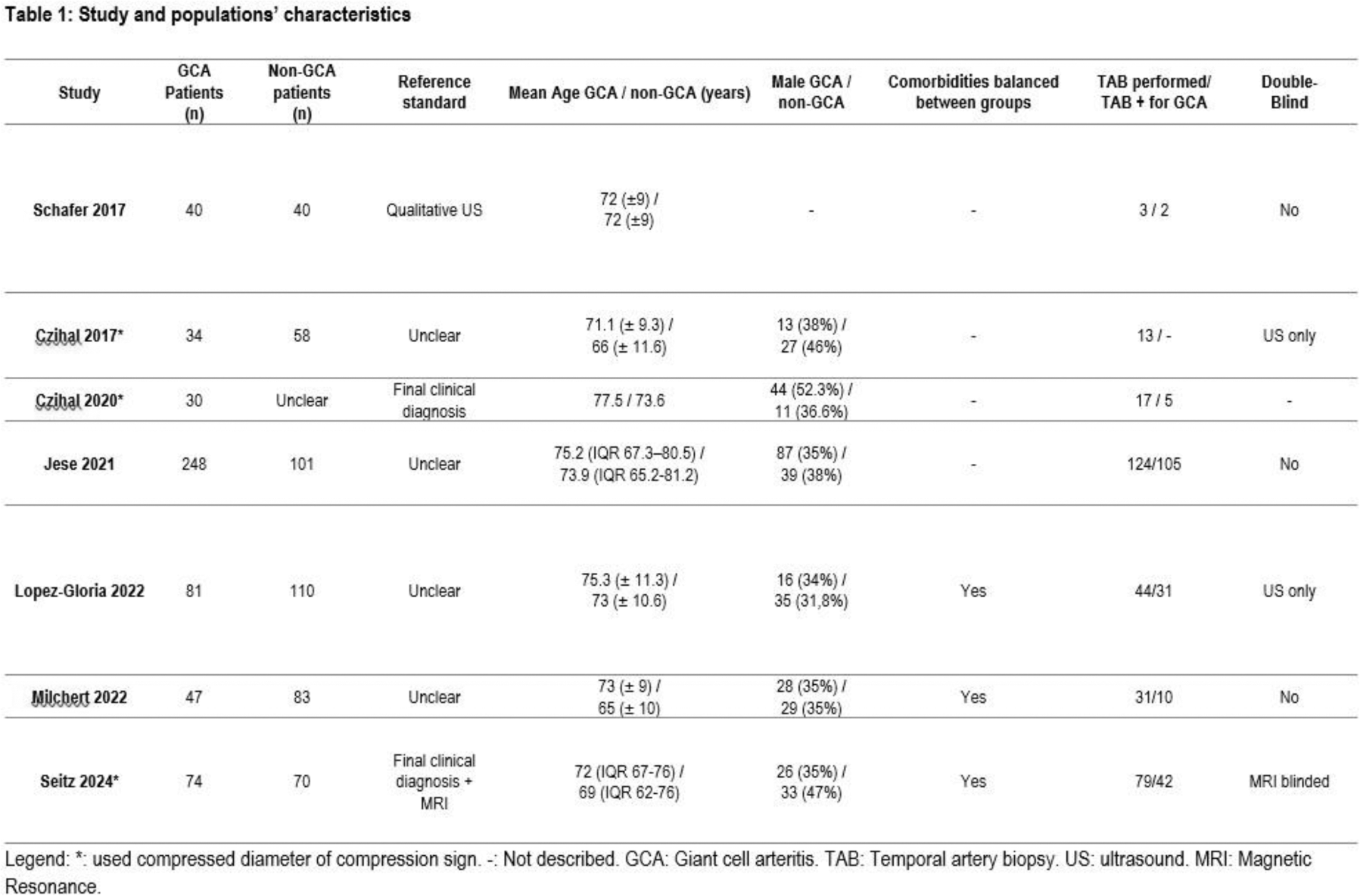
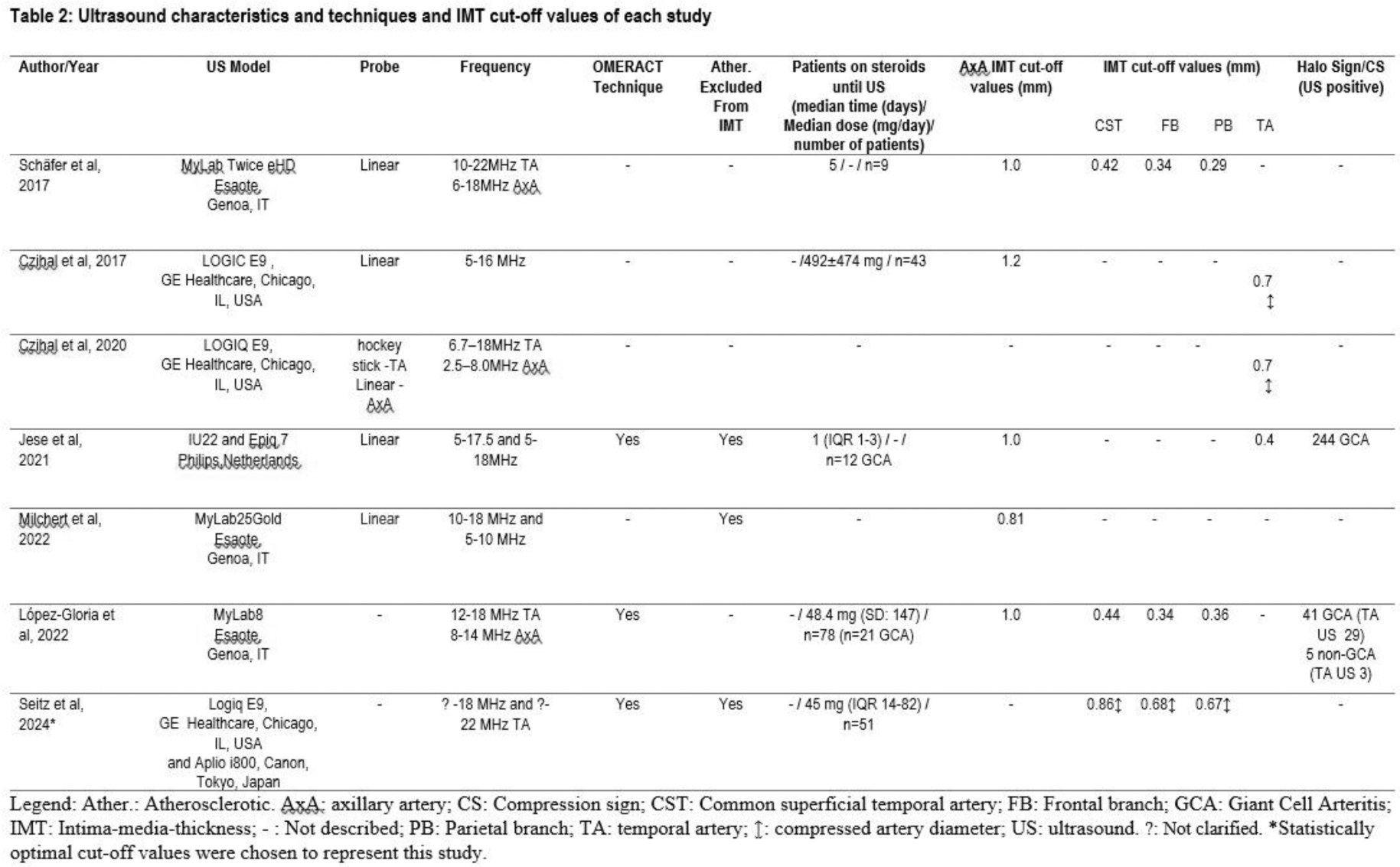
Results: Among 2786 records screened by title and abstracts, 7 fulfilled the inclusion criteria. A total of 1150 patients were included; the mean age of the patients in the different studies ranged from 67.8 to 74.8 years. The proportion of male/female was balanced. 554 patients had a final diagnosis of GCA, as shown in Table 1. Only three studies described cardiovascular risk factors or presence of cardiovascular disease of the patients. In one of these studies, individuals with high/very high cardiovascular risk needed higher IMT cut-off values (1.03 mm vs. 0.84 mm for the common superficial temporal artery stem, 0.86 mm vs. 0.71 mm for the frontal branch, and 0.80 mm vs. 0.63 mm for the parietal branch) for achieving an appropriate diagnostic accuracy for GCA. In another study, the specificity of the cut-off (0.7 mm compression diameter of compression sign) was lower in males over 70 years-old with 70% compared to 84.5% in the overall population. The proposed IMT cut-off values for vasculitis in the studies varied between 0.81 and 1.2 mm for the axillary artery (Axa). The IMT cut-off values for temporal artery (TA) were heterogeneously described. Three studies provided a single cut-off value for the TA with 0.4mm for IMT and 0.7 mm for compressed diameter. The remaining three studies reported cut-off values for individual TA branches, showing values of 0.42-0.44mm for IMT and 0.86mm for compressed diameter in the stem, and 0.29–0.36mm for IMT and 0.67mm for compressed diameter in the parietal and 0.34 mm for IMT and 0.68 mm for compressed diameter in the frontal branch (Table 2). The reported diagnostic accuracy of the IMT cut-off values used for both TA and the Axa, was high across all studies (sensitivities: 76 to 100%, specificities: 85.7 to 100%). The high reported sensitivities strongly suggest that the reference standard in these studies was not the final diagnosis of GCA (which in clinical practice is lower due to the segmental nature of the disease) but the result of detecting thickened IMT in GCA affected segments (which can ideally be 100%), i.e. qualitative judgement in US of the respective segment or the result of MRI visible affections of the vessel segment. All studies have a high risk of bias in at least two QUADAS-2 domains due to patient selection issues, lack of US blinding, and use of the index test as part of the reference standard. Another major drawback was that non-vasculitic factors potentially influencing IMT, such as age, sex and the presence of cardiovascular risk factors were considered only in two studies. The studies also showed variability in steroid doses and duration before US, which could have influenced diagnostic accuracy.
Conclusion: Valid IMT defined cut-off levels for diagnosing GCA in the TA and Axa in clinical routine are not yet available. Further unbiased research, taking non-vasculitic factors for IMT thickening into consideration, is needed.
REFERENCES: NIL.
Acknowledgements: Centro de Estudos em Reumatologia Pedro Ernesto (CERPE) - University of the State of Rio de Janeiro.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (