fetching data ... 
Background: Recent evidence disclosed increased cardiovascular disease (CVD) risk in not only inflammatory rheumatic diseases but also osteoarthritis (OA) and fibromyalgia (FM). OA and FM are mostly viewed as non-inflammatory rheumatic conditions. However, increased inflammatory cytokine and C-reactive protein (CRP) production as well as reduced anti-inflammatory cytokine levels are now well documented in both OA and FM [1, 2]. Cumulative systemic inflammation induced by characteristically fluctuating disease activity over time enhances CVD risk among patients with RA. Notably in the present context, disease activity scores in 28 joints (DAS28) have previously been employed in FM [3]. Whether systemic inflammation and DAS28 impact CVD risk in OA and FM awaits elucidation.
Objectives: We compared the potential impact of inflammation markers and DAS28 on atherosclerosis among patients with RA, OA and FM.
Methods: We recorded high sensitivity (hs)-CRP concentrations and erythrocyte sedimentation rates (ESR), calculated the DAS28-CRP and DAS28-ESR and performed detailed carotid and femoral artery high resolution ultrasound in 332 consecutive patients. These included 107 patients with RA, 165 with OA and 60 with FM; 73.0% were white, 17.1% Asian, 9.6% black and 0.3% of mixed ancestry. Ultrasound measures comprised carotid and femoral artery prevalence, number and area as well as mean carotid intima-media thickness (cIMT). The Framingham score was used as an index of the overall traditional cardiovascular risk factor burden. The data were analysed in age, sex and black population origin adjusted multivariate regression models unless indicated otherwise.
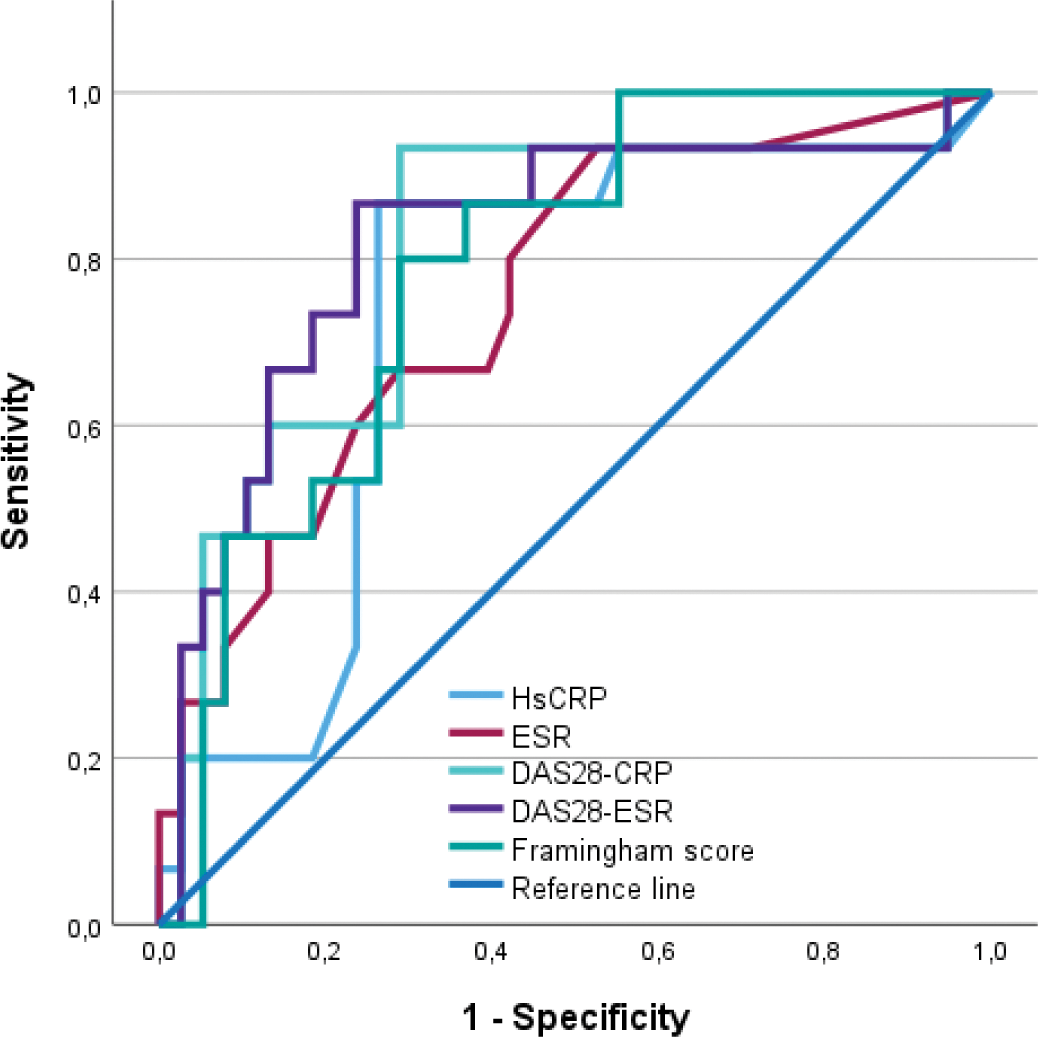
Results: Median (interquartile range) hs-CRP levels and ESR were larger (p<0.001 for both) in RA patients (3.5 (1.1-17.0) mg/l and 13 (4-30) mm/hr) than in those with OA (2.1 (0.8-5.3) mg/l and 6 (3-15) mm/hr) or FM (3.0 (0.9-6.8) mg/l and 9 (3.5-13.0) mm/hr); mean (SD) DAS-CRP and DAS-ESR were larger (p<0.001 for both) in patients with RA (3.5 (1.4) and 3.6 (1.6)) than in those with OA (2.1 (0.9) and 2.1 (1.2)) or FM (2.0 (1.0) and 1.9 (1.2)). Atherosclerosis measures did not differ (p>0.05 for all) among RA, OA and FM patients. In all patients, acute phase responses and DAS28 were not associated (p=0.053-0.978) with plaque prevalence, number and area and cIMT. FM impacted the relationships of hs-CRP (interaction p=0.014), ESR (interaction p=0.003), DAS28-CRP (interaction p=0.019) and DAS28-ESR (interaction p=0.040) with plaque prevalence. FM also influenced the relationships of ESR (interaction p=0.002) and DAS-ESR (interaction p=0.002) with plaque number. Accordingly, as given in Table 1, inflammation markers and DAS28 values were strongly associated with plaque prevalence in patients with FM but not in those with RA or OA. These relationships were consistently unaltered after additional adjustment for the Framingham score and remained significant (p< 0.037 for all) after adjustment for body mass index or waist circumference. Figure 1 shows that inflammation markers and DAS28 values performed as well as the Framingham sore in identifying FM patients with plaque. Intergroup comparisons of the areas under the curves (0.732 to 0.821) revealed no differences (p=0.118 to 0.842).
Conclusion: One point in time measured levels of systemic inflammation markers and disease activity scores in 28 joints evaluations are strongly associated with very high risk atherosclerosis in FM but not OA and RA patients. These potential atherogenic effects are not mediated by major traditional CVD risk factors or/and adiposity. Our results suggest that systemic inflammation in patients with FM can mediate enhanced CVD risk.
REFERENCES: [1] Molnar V, Int J Mol Sci, 2021.
[2] Rodriguez-Pino et al, Immunol Lett, 2014.
[3] Leeb BF, Rheumatol, 2004.
Associations of inflammation markers and DAS28 values with atherosclerosis measures that differed among rheumatic conditions.
| Any plaque presence
|
||||
|---|---|---|---|---|
| Characteristics | RA | OA | FM | Interactions |
| ESR | 1.01 (0.98-1.03), 0.594 | 1.01 (0.98-1.04), 0.612 | 1.20 (1.06-1.35), 0.003 | FM with p =0.003 |
| 1.10 (1.02-1.18), 0.013 a | ||||
| Hs-CRP | 1.00 (0.999-1.02), 0.880 | 0.94 (0.87-1.02), 0.147 | 1.18 (1.03-1.37), 0.021 | FM with p =0.014 |
| 1.12 (1.01-1.25), 0.038 a | ||||
| DAS28-ESR | 1.02 (0.77-1.35),0.873 | 1.33 (0.95-1.88), 0.100 | 2.32 (1.25-4.32), 0.008 | FM with p =0.040 |
| 2.64 (1.40-5.00), 0.003 a | ||||
| DAS28-CRP | 0.99 (0.72-1.37), 0.970 | 1.27 (0.86-1.89), 0.224 | 2.27 (1.16-4.16), 0.017 | FM with p =0.019 |
| 2.76 (1.37-5.60), 0.005 a | ||||
Associations were assessed in age, sex and black population origin adjusted regression models unless indicated otherwise. Significant associations are given in bold. OR, odds ratio; CI, confidence intervals; RA, rheumatoid arthritis; OA, osteoarthritis; FM, fibromyalgia; ESR, erythrocyte sedimentation rate; hs-CRP, high sensitivity C-reactive protein; DAS28-ESR, disease activity score in 28 joints using ESR; DAS28-CRP, disease activity score in 28 joints using CRP. a Adjusted for Framingham and black population origin.
The performance of inflammatory markers and DAS28 values compared to the Framingham score in the identification of fibromyalgia patients with carotid or/and femoral artery plaque. AUC=area under the curve; Hs-CRP=high sensitivity C-reactive protein; ESR=erythrocyte sedimentation rate; DAS28-CRP disease activity score in 28 joints using CRP; DAS28-ESR=disease activity score in 28 joints using ESR.
Acknowledgements: Not applicable.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (