fetching data ... 
Background: Follow-up of autoimmune inflammatory rheumatic diseases (AIIRD) is a challenging task due to the need for clinical assessment and lack of a reliable remote monitoring method. Patient-reported outcomes (PROMs) are widely used, but their results may be biased by comorbidities, especially those causing pain. PROMs outcomes depend on the patient’s personality and require some insight into their illness. If well-tuned, PROMs surveys give trustworthy results, although completing them can be time-consuming and monotonous. The main goal of our project is to develop an automated system for remote monitoring of AIIRD patients. We have chosen the analysis of a signal from a single accelerometer due to its availability, low cost and minimal intrusion into privacy. The proposed future equipment can be, for example, worn as a watch. In this work, we present results from a proof-of-concept study.
Objectives: To evaluate the usefulness of accelerometry signal from a single device in estimating the DAS28-ESR score as a part of arthritis activity evaluation.
Methods: We have included 30 patients with rheumatoid arthritis (24) and psoriatic arthritis (6). The patients had no significant comorbidities. There were 20 women and 10 men enrolled. The mean age was 59.5 years (min. 40 - max. 74 years). Participants were asked to perform different activities: clapping, walking, sitting, lifting arms, etc. However, for this study, we analyzed accelerometry signals only from 3 minutes of clapping. The signal was divided into 3-second samples, and 54 numerical features were subsequently extracted. The features list included autoregression coefficients, median absolute deviation (MAD), variance, Fourier’s components, entropy, kurtosis, skewness and others. Samples were divided into training and testing datasets in a ratio of 80:20. We built all models using Bayesian regularisation for a feed-forward neural network algorithm (BRNN). We performed all analysis with R version 4.4.2, using package “brnn”. We created two main models - the first only with features extracted from accelerometry (model A) and the second with the features and global patient assessment (GPA) in visual analogue scale (model B). The efficacy of the models was tested, making predictions of DAS28-ESR from the testing dataset. We used root mean square error (RMSE) as a primary performance parameter. We analyzed the effectiveness in predicting DAS28-ESR remission from samples. The remission was defined as DAS28-ESR equal to or below 2.6. We used accuracy with sensitivity and specificity as an efficacy measure. Because GPA is a component of the DAS28 score, we built a BRNN model with only GPA as a predictor. We tested the predictive power of this model separately. The local authorities accepted the study, and all participants signed the informed consent form.
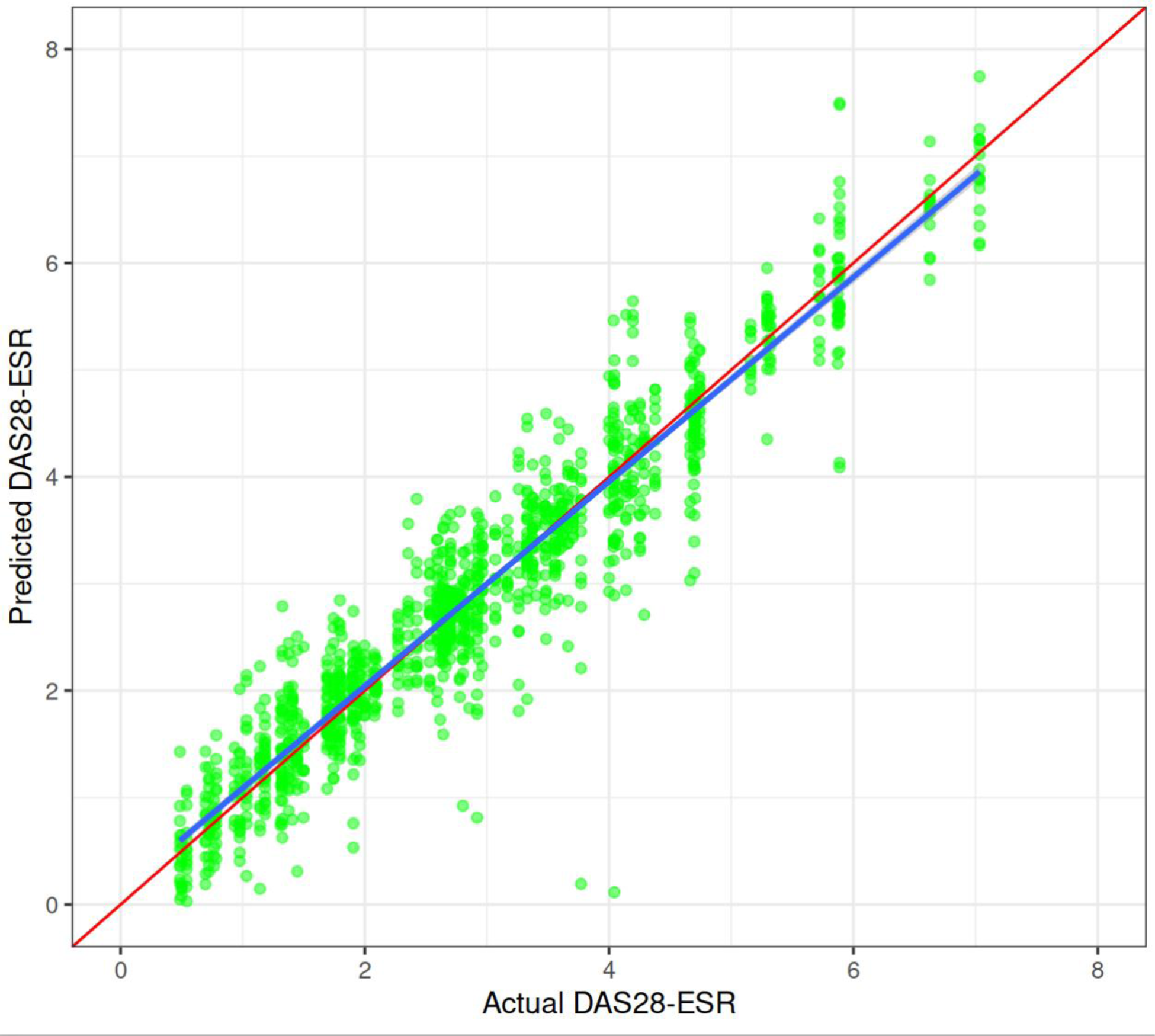
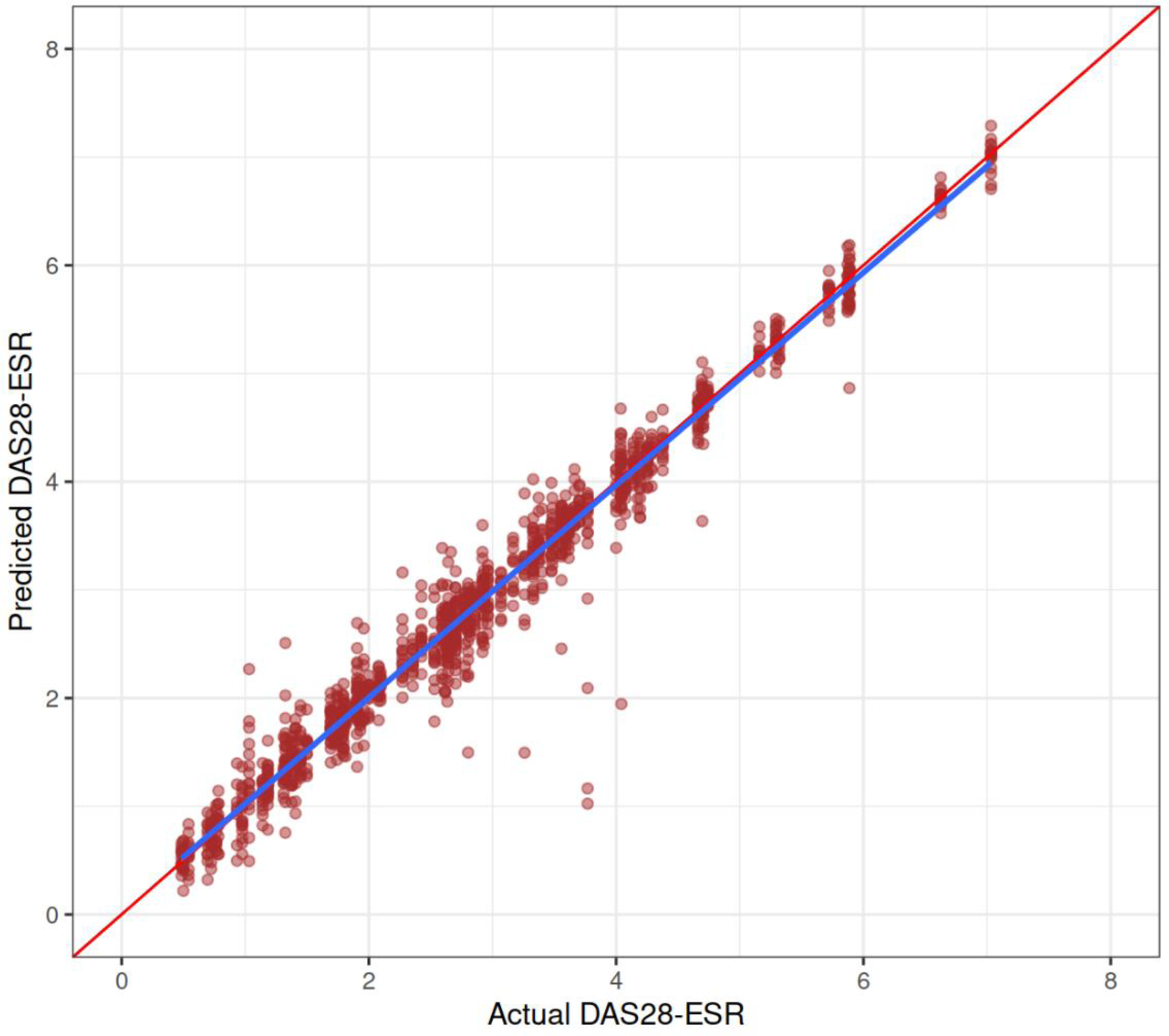
Results: Both main models performed well, with better DAS28-ESR prediction of model B, as expected. RMSE for models A and B was 0.48 (95% CI 0.463-0.5) and 0.255 (95% CI 0.246-0.266), respectively. Accuracy, sensitivity and specificity in predicting DAS28-ESR remission were 0.904/0.938/0.861 for model A and 0.922/0.965/0.871 for model B. The model with GPA as a single predictor worked worse with RMSE 0.668 (95% CI 0.643-0.695). Figures 1 and 2 show DAS28-ESR predictions from models A and B.
DAS28-ESR estimation for model A in the test dataset. The X-axis shows the actual DAS28-ESR and the Y-axis shows the estimation. Each point depicts the result of one sample. The red oblique line shows ideal fitting. The blue line shows the mean of estimated values. Light blue shadows represent standard error.
DAS28-ESR estimation for model B in the test dataset. See the Figure 1 caption for further explanations.
Conclusion: Accelerometry is a potentially helpful tool for predicting the DAS28 score. The method could be used in a remote follow-up of arthritis patients. This is a proof-of-concept study, and the results need further evaluation. One can expect a negative impact of comorbidities on arthritis activity score prediction. However, additional models or data tuning can increase the efficacy of models.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (