fetching data ... 
Background: Cardiovascular diseases (CVD) are a significant concern in autoimmune conditions like Familial Mediterranean Fever (FMF), marked by ongoing subclinical inflammation. Colchicine has an antiinflammatory effects on cardiovascular (CV) system and it is used lifetime in FMF.
Objectives: To evaluate the CV risk and the colchicine’s effect on it in patients with FMF.
Methods: This study is a prospective, cross-sectional study involving patients diagnosed with FMF according to the Tel-Hashomer criteria. Demographic and clinical characteristics were recorded. Colchicine dosage, duration of use, and observed side effects related to colchicine use documented. Family history of FMF, IL-1 inhibitor use, number of attacks in the last 3 and 6 months, and attack characteristics were also recorded. Gene analysis results were noted. CV risk factors including hypertension, diabetes mellitus, and hyperlipidemia were recorded. The Framingham Risk Score was calculated. Because of CV Risk Score was validated for persons over 30 years old we grouped our patients according to this age limit for some analysis. Laboratory values were also noted, including erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) serum amyloid A (SAA).
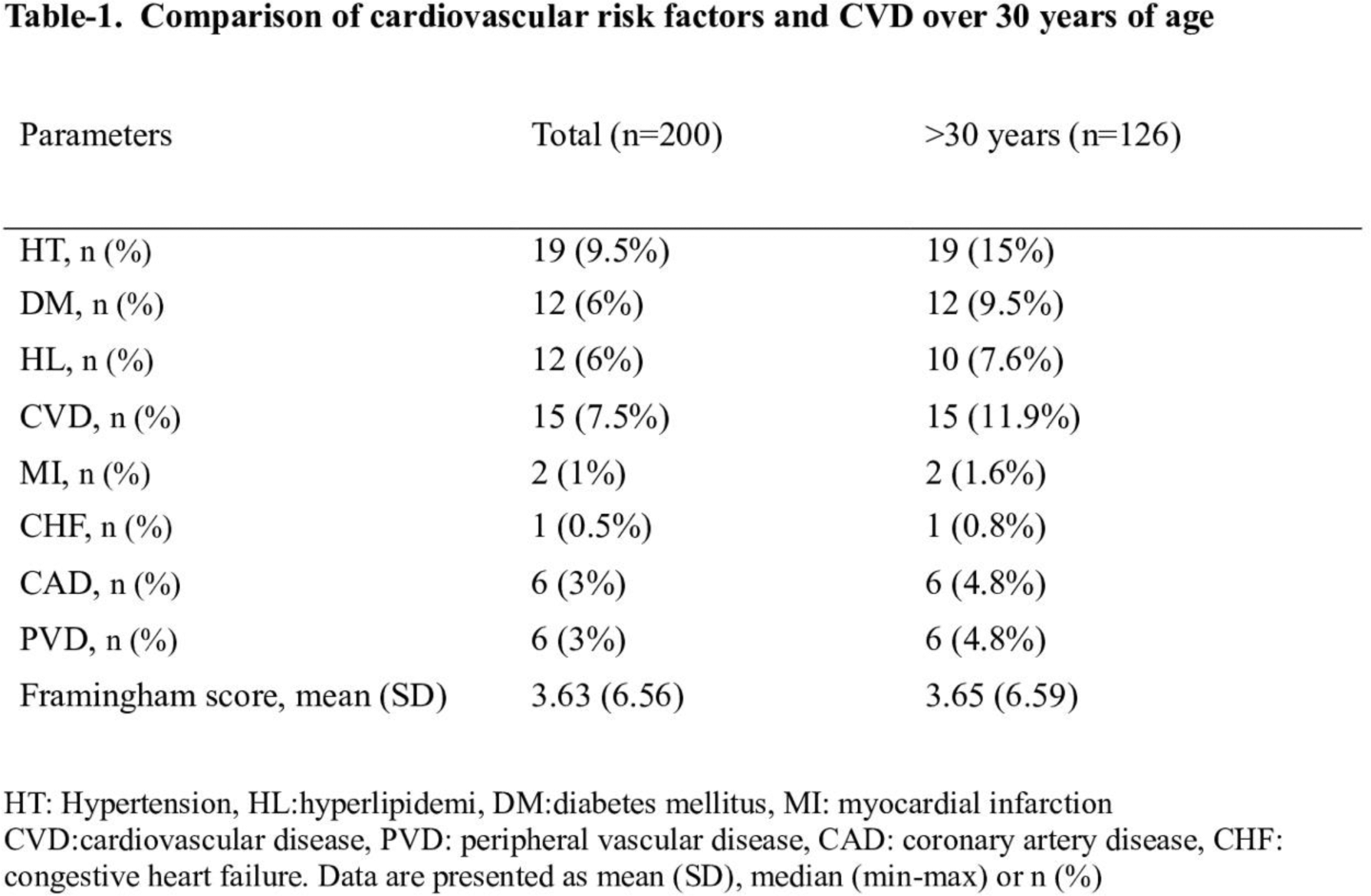
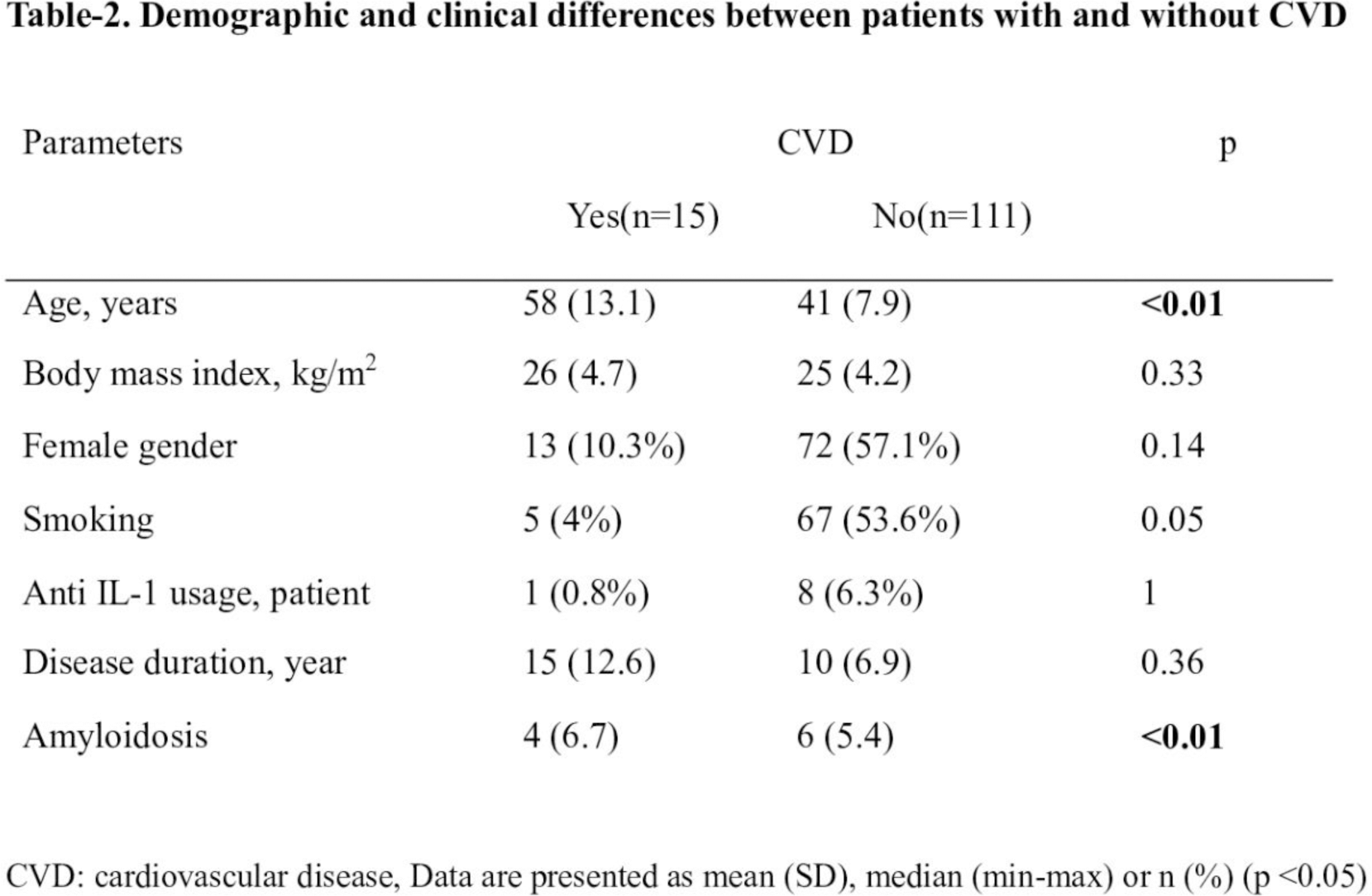
Results: The study included 200 patients with a mean age of 36 (SD: 12.9) years, of whom 121 (60.5%) were women. The mean symptom duration was 12.7 (SD:8.9) years, disease duration was 9.4 (SD:7.4) years. The mean BMI of the patients was 24.9 (SD: 4.2), with 25 (12%) obese. 106 (53%) of the patients were currently smoking. All patients were using colchicine, while 11 (5.5%) were using IL-1 inhibitors. The mean colchicine dosage was 1.45 (SD: 0.83), with colchicine resistance observed in 14 patients (7%) and colchicine side effects in 1 patient (0.5%). The mean number of attacks in the last 3 months was 1 (0-4), while in the last 6 months, it was 1 (0-6). In the genetic analysis results, the M694V homozygote was 23 (11.5%), M694V heterozygote was 21 (10.5%). CVD was present in 15 (7.5%) patients; of these, 2 (1%) were myocardial infarction (MI), 1 (0.5%) was congestive heart failure, 6 (3%) were coronary artery disease, and 6 (3%) were peripheral vascular disease. The mean Framingham Score was 3.63 (SD: 6.56) (Table 1). There were no patients with CVD age below 30 years old. Assessing the difference between patients aged >30 with and without CVD, age and amyloidosis was found to be statistically significant (p <0.01) (Table 2). In the multivariate regression analysis related to CVD, age, gender, smoking status, disease duration, cumulative colchicine dose, amyloidosis and serum CRP level were evaluated. Amyloidosis (OR:55.7) and age (OR:1.2) were statistically significant (p<0.05).
Conclusion: Age and amyloidosis were found to be associated with CVD in FMF. We did not find any significant difference between other CV risk factors and the cumulative dose of Colchicine. To use of colchicine may have a cardioprotective effect by reducing amyloidosis. More extensive and prospective studies are needed in this area.
REFERENCES: [1] Alsarah A, Alsara O, Laird-Fick HS. Cardiac manifestations of Familial Mediterranean fever. Avicenna J Med. 2017;7(4):158-63.
[2] Canpolat U, Dural M, Aytemir K, Akdogan A, Kaya EB, Sahiner L, et al. Evaluation of various cardiac autonomic indices in patients with familial Mediterranean fever on colchicine treatment. Auton Neurosci. 2012;167(1-2):70-4.
[3] Imazio M. Contemporary management of pericardial diseases. Curr Opin Cardiol. 2012;27(3):308-17.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (