fetching data ... 
Background: Cardiovascular (CV) risk is increased in patients with systemic sclerosis (SSc) due to systemic inflammation and vascular impairment leading to accelerated atherosclerosis (ATS). Current tools for CV risk calculation underestimate the risk in SSc.
Objectives: This study aimed to test the accuracy of SCORE and SCORE2 for the general population, its modification for inflammatory arthropathies (recommended by EULAR), and a new potential coefficient.
Methods: 92 SSc patients (81 females; mean age 52; mean disease duration 6.8 years; dcSSc: n=28, lcSSc: n=64) and 197 HC (147 females, mean age 56.7) with no history of CV disease (angina pectoris, myocardial infarction, cerebrovascular, and peripheral arterial events) were included. Disease activity and clinical features were evaluated in SSc. All participants underwent examinations of carotid artery disease (CARD), carotid intima-media thickness (CIMT), pulse wave velocity (PWV), ankle-brachial index (ABI), and body composition (by densitometry and bioelectrical impedance analysis). Comorbidities and current medication were recorded. The risk of fatal CV events was evaluated by the Systematic COronary Risk Evaluation (SCORE) and SCORE2, in SSc also by the modified (mSCORE) by coefficient 1.5 as recommended by EULAR for inflammatory arthritis, and 3.59 (SCOREx3.5; SCORE2x3.5) based on the estimated CV risk in SSc [1].
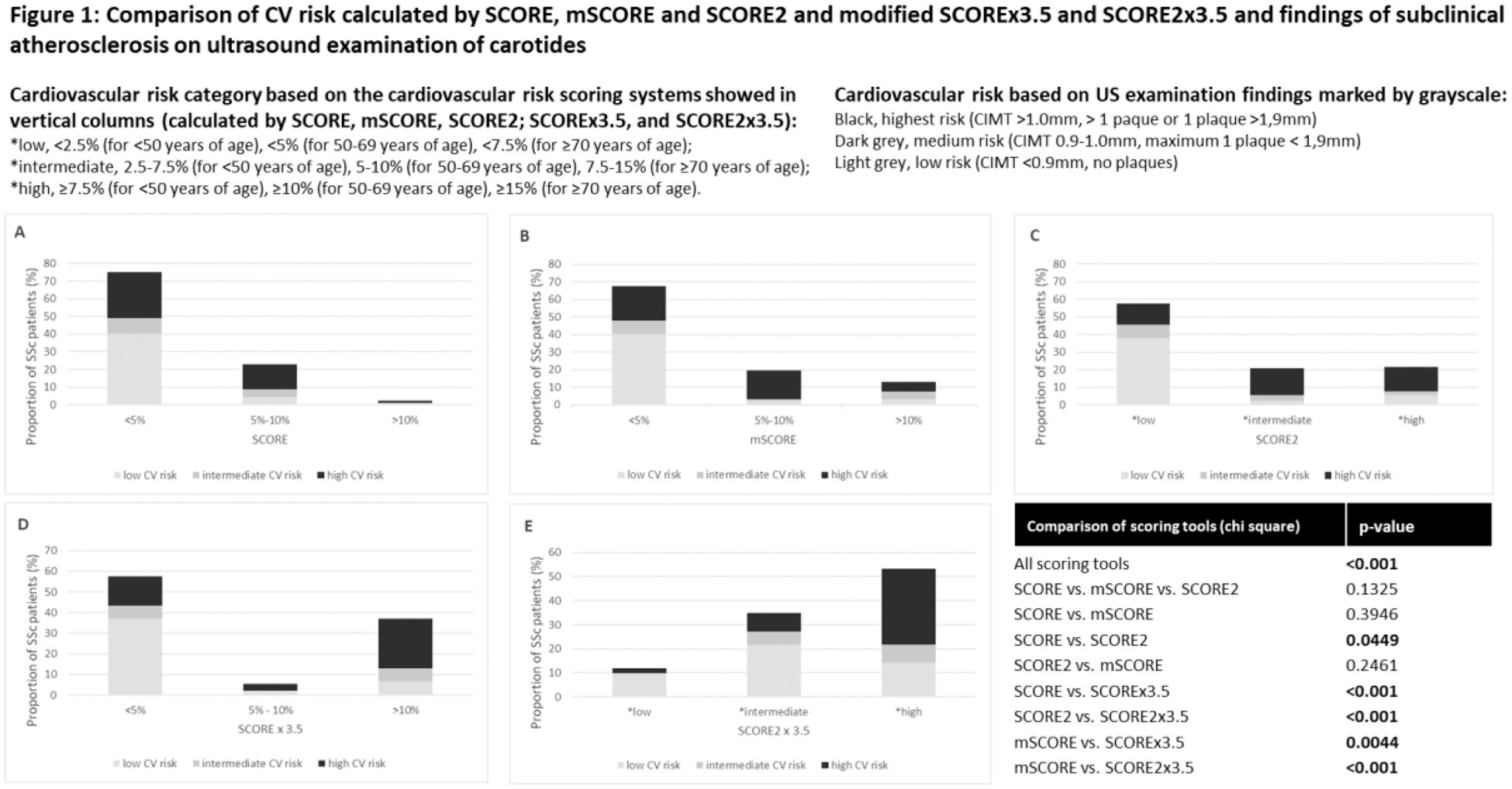
Results: SSc patients had a trend to more prevalent dyslipidemia (p=0.063) and significantly more often prediabetes (p<0.001), but a comparable prevalence of arterial hypertension, diabetes mellitus, and current smoking to HC. Nevertheless, SSc used significantly more frequently antihypertensives than HC (p<0.001), including vasoactive treatment by calcium channel blockers. SSc had a significantly increased prevalence of CARD, unfavorable CIMT, and ABI (p<0.05 for all), and a trend to lower SCORE, but no significant difference in SCORE2 compared to HC. On the contrary, the overall CV risk based on US examination (CARD, CIMT) was significantly higher in SSc. In SSc, the CV risk and markers of subclinical ATS were associated especially with age, HbA1c, disease duration, and mean arterial pressure (p<0.05 for all). A comparison of calculated CV risk with US examination showed inaccuracy of the SCORE, mSCORE, and SCORE2. On the other hand, the modification of SCORE and SCORE2 by coefficient 3.59, showed significantly higher accuracy in the estimation of CV risk, when compared to the carotid US finding (Figure 1).
Conclusion: This cross-sectional case-control study demonstrated a significantly increased risk of subclinical ATS in SSc compared to HC, although there was an opposite trend in CV risk estimated by calculated SCORE. The CV risk in SSc was associated especially with age, disease duration, and HbA1c levels. Scoring systems SCORE and SCORE2 recommended for the European general population underestimated the CV risk when compared to the US examination. Using the coefficient 3.59 based on estimated CV risk for SSc [1] significantly increases the accuracy of available CV risk scoring systems.
REFERENCES: [1] Conrad N et al. Lancet. 2022;400(10354):733-743.
Acknowledgements: MHCR (023728), Biobanks and Biomolecular Resources Research Infrastructure Consortium (BBMRI-CZ LM2018125).
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (