fetching data ... 
Background: Aortic aneurysms and/or aortic dissection are severe vascular complications that can be due to an underlying inflammatory disease, such as Giant Cell Arteritis (GCA) [1–3].
Objectives: In biopsies of aortic samples of patients undergoing cardiovascular surgery we assessed: a ) pathological inflammatory and non-inflammatory pattern, b ) association with an underlying inflammatory entity.
Methods: We reviewed the aortic samples of patients undergoing cardiovascular surgery due to aortic aneurysms and/or aortic dissection from January 2017 to December 2018 and from February 2022 to December 2023 in a University referral hospital. Biopsies were differentiated into inflammatory and non-inflammatory pattern. Inflammatory pattern was considered by the presence of inflammatory histological findings in any of the aortic layers. Biopsies were analysed by an expert pathologist. In addition, all the clinical records and patients were studied by a rheumatologist to rule out an underlying inflammatory disease previously, at that moment or surgery or in the follow-up.
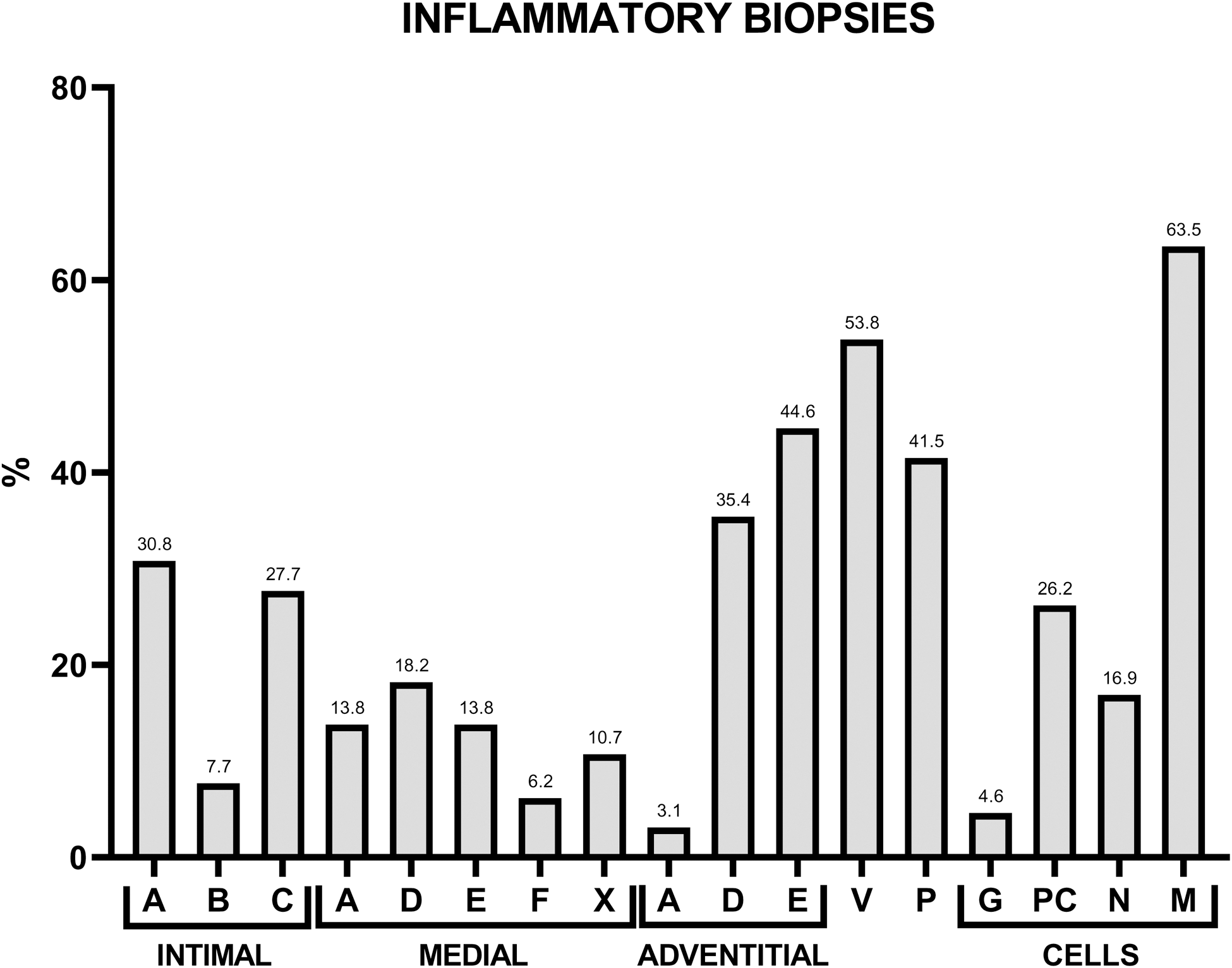
Results: We studied 97 patients (77 men/20 women); mean age of 63.4±11.2 years) who had undertaken a surgery for aortic aneurysm and/or aortic dissection. The samples corresponded to thoracic aortic aneurysm (n=88; 90.7%), abdominal aortic aneurysm (n=2; 2.1%), and aortic dissection without previous aneurysm (n=7; 7.2%). Pathologic patterns were inflammatory (n=65; 67%) and non-inflammatory (n=32; 23 %). The main characteristics of these patients are listed in Table 1. There was no demographic, cardiovascular risk factors, clinical and analytical findings between both groups (pathological inflammatory vs non-inflammatory). Nineteen (19,6%) patients died; during cardiovascular surgery (n= 14) and in follow-up (n= 5). The main histological findings of 65 patients with inflammatory pattern are summarized in Figure 1. Two common findings were identified, vasa vasorum involvement (n=35; 36.8%) and periaortic fibrosis (n=27; 28.4%). The presence of giant cells was observed in 3 (3.2%) patients, none of them had GCA, nor developed GCA. The study for an underlying inflammatory disease showed 2 (2%) patients previously diagnosed with GCA and 1 patient (1.1%) with GCA diagnosed after surgery postoperatively. Two of 3 patients had an inflammatory pattern with vasa vasorum involvement and periaortic fibrosis; however, the other previously diagnosed had a non-inflammatory pattern. No other patients suffered from an inflammatory disease after the surgery.
Conclusion: In our study, most patients who undergo surgery for an aortic aneurysm and/or aortic dissection do not have and will not have an inflammatory disease, regardless of the presence of inflammatory findings in the biopsy.
REFERENCES: [1] Martín-Gutiérrez A, et al. Eur J Intern Med. 2024 Nov; 129:78-86. doi: 10.1016/j.ejim.2024.06.013.
[2] Loricera J, et al. Clin Exp Rheumatol. 2015 Mar-Apr; 33(2 Suppl 89): S-19-31. PMID: 25437450.
[3] Loricera J, et al. Clin Exp Rheumatol. 2014 May-Jun;32(3 Suppl 82):S79-89.
Main characteristics of 97 aortic biopsies. Data are considered at the moment of surgical procedure. Comparison between patients with inflammatory and non-inflammatory aortic biopsies.
| Overall
| Inflammatory
| Non-Inflammatory
| p | |
|---|---|---|---|---|
| General features | ||||
| Age (mean±SD) at diagnosis
| 63.4±11.2
| 63.3±9.8
| 63.5±13.9
| 0.932
|
| Cardiovascular risk factors | ||||
| High blood pressure, n (%) | 59 (61.5) | 41 (64.1) | 18 (56.3) | 0.509 |
| Dyslipidemia, n (%) | 46 (47.9) | 34 (53.1) | 12 (37.5) | 0.194 |
| Diabetes, n (%) | 16 (16.7) | 13 (20.3) | 3 (9.4) | 0.248 |
| Previous or current smoking history, n (%) | 53 (55.2) | 38 (59.3) | 15 (46.9) | 0.281 |
| Heart attack, n (%) | 6 (6.3) | 4 (6.3) | 2 (6.3) | 0.999 |
| Stroke, n(%) | 5 (5.2) | 3 (4.7) | 2 (6.3) | 0.999 |
| Location of biopsy | ||||
| Thoracic aneurysm | 88 (90.7) | 58 (89.2) | 30 (93.8) | 0.713 |
| Abdominal aneurysm | 2 (2.1) | 2 (2.1) | 0 (0) | 0.999 |
| Dissection without aneurysm | 7 (7.2) | 5 (7.7) | 2 (6.3) | 0.999 |
| Symptoms at surgery | ||||
| Chest pain, n (%) | 27 (28.1) | 18 (28.1) | 9 (28.1) | 0.999 |
| Dyspnea, n (%) | 38 (39.6) | 23 (35.9) | 15 (46.9) | 0.377 |
| Asymptomatic, n (%) | 36 (37.5) | 24 (37.5) | 12 (37.5) | 0.999 |
| Rheumatological manifestations | ||||
| Scalp tenderness, n (%) | 1 (1) | 1 (1.6) | 0 (0) | 0.999 |
| PmR, n (%) | 2 (2.1) | 1 (1.6) | 1 (3.1) | 0.999 |
| Jaw claudication, n (%) | 0 (0) | 0 (0) | 0 (0) | 0.999 |
| Acute phase reactants | ||||
| CRP (mg/dL), median [IQR] | 0.4 [0.4-0.4] | 0.4 [0.4-0.9] | 0.4 [0.4-0.4] | 0.393 |
| Aneurysm size, n (% ) | 53.3±12.9 | 55±15.4 | 50.2±4.9 | 0.042 |
| Dissections, n (% ) | 18 (18.6) | 13 (20) | 5 (15.6) | 0.783 |
| Deaths, n (% ) | 19 (19.6) | 10 (15.4) | 9 (28.1) | 0.175 |
Abbreviations : bDMARDs: biological disease modifying antirheumatic drugs; CRP: C-reactive protein; GCA: giant cell arteritis; IQR: interquartile range; scDMARDs: synthetic conventional disease modifying antirheumatic drugs; n: number;SD: standard deviation.
Main pathological findings in biopsies of 65 samples with inflammatory pattern.
Abbreviations : A: inflammation; B:fibrosis; C: fibrosis plus inflammation; D: atheromatosis; E: atheromatosis with inflammation; F: dissection; G: giant cells; M: macrophages; N: neutrophils; P: periaortic fibrosis; PC: plasma cells; V: vasa vasorum inflammations; X: myxoid degeneration.
Acknowledgements: NIL.
Disclosure of Interests: Adrián Martín-Gutiérrez: None declared, Javier Loricera: None declared, Jose María Gómez-Ortega: None declared, Ander Ucelay: None declared, Ricardo Blanco AbbVie, Pfizer, Roche, GSK, Lilly, UCB, BMS, Novartis, Janssen, UCB and MSD.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (