fetching data ... 
Background: White or green light is traditionally used to image capillaries at the nailfold to enable good contrast between the capillaries and surrounding tissue. Anecdotally, visualising nailfold capillaries is challenging in darker skin tones due to the absorption of light by melanin in the epidermis, obscuring the view of capillaries below in the dermis. This often means that capillaries cannot be observed.
Objectives: The study aimed to make capillaroscopy more inclusive and suitable for all. Our objective was to quantify the difficulty in visualising capillaries in darker skin tones and specifically to test the hypothesis that using ultraviolet or infrared light improve visualisation of the capillaries in darker skin tones.
Methods: Participants were healthy controls across all six categories of Fitzpatrick skin type (I [Burns easily and does not tan, lighter skin tone] -VI [Never burns, always tans darkly, darker skin tone]). They underwent capillaroscopy imaging on the ring finger of both hands with four handheld nailfold capillaroscopy microscopes, each illuminated by an LED of different wavelengths: green, white, infrared and ultraviolet. For each camera and finger, a second blinded observer manually marked all visible capillaries in a single representative frame. For each camera the number of capillaries (capillary count) per image was assessed. Mixed-effects Poisson regression was used to model the capillary counts across all cameras. The model included mean capillary count (number of capillaries per image) as the outcome, with Fitzpatrick skin type, camera type, and a skin-type-by-camera-type interaction effect as predictor variables. A random effect for participant identifier was also included to account for the nested nature of the dataset.
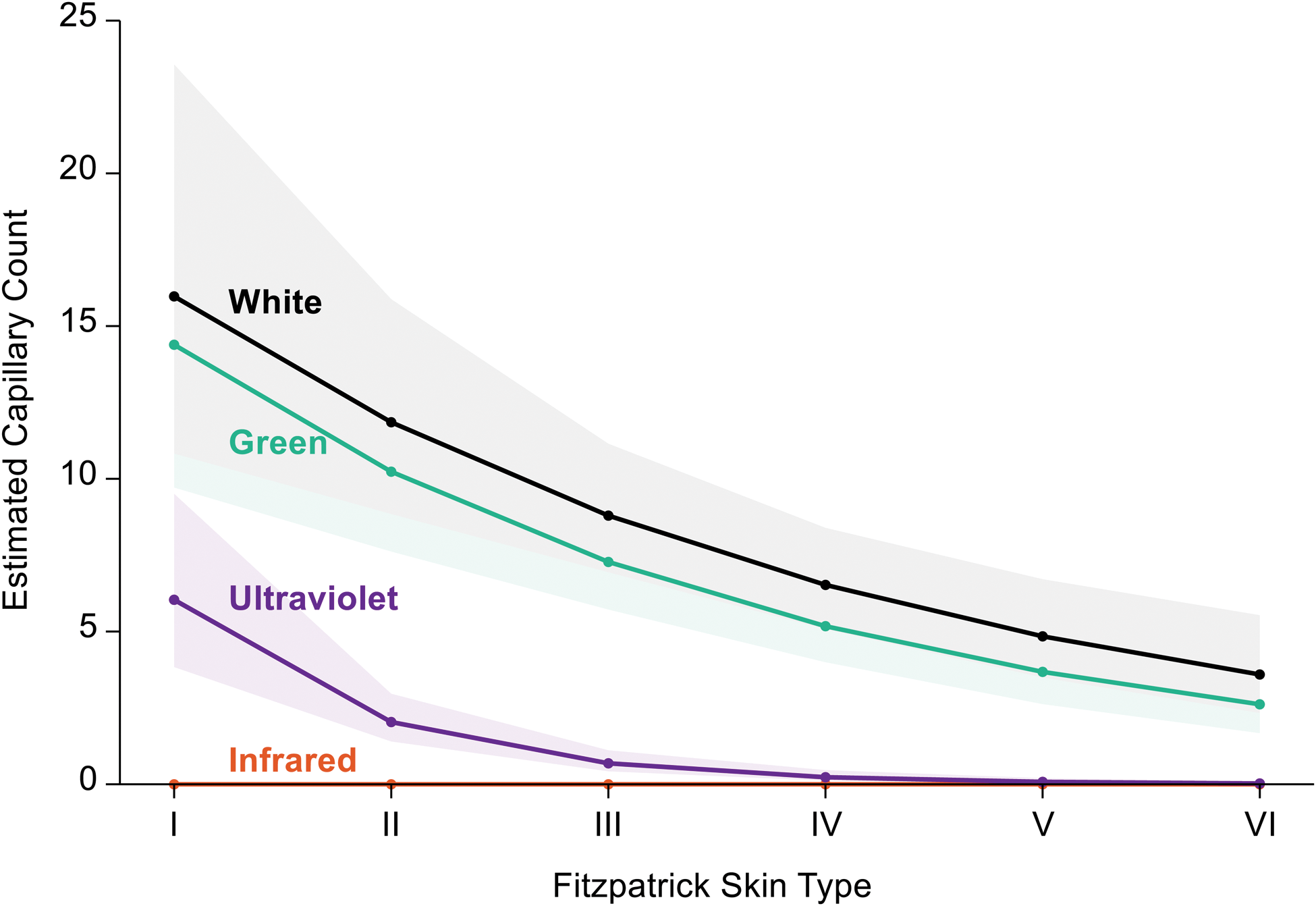
Results: There were 25 participants (median age 32 years (IQR 28 to 44), 16 (64.0%) female. Eight participants had a Fitzpatrick skin tone category of type I or II (32.0%); 8 (32.0%) type III or IV, and 9 (36.0%) type V or VI. Capillary count was greatest with the white and green light microscopes, returning a significantly higher mean capillary count in the same participants than the ultraviolet and infrared microscopes (Figure 1, Table 1). Ultraviolet and infrared microscopes did not offer enough contrast to observe/count the same capillaries as observed with the white and green camera, with no capillaries being observed with the infrared microscope. With respect to Fitzpatrick skin type, all microscopes found statistically significantly fewer capillaries as skin type increased, with the white and green microscope following similar diminishing trends, and the ultraviolet microscope having a steeper falloff with increased skin darkness. For the white light camera, the median capillary count dropped from 18.3 in skin type I to 4.1 in skin type V; for the green camera, capillary count fell from 16.5 to 3.0 from types I to VI.
Capillary count per image by skin type, taken from the mixed-effects poisson model
| Camera | Fitzpatrick Skin Type | |||||
|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | |
| White | 18.3 (10.8 to 25.9) | 13.6 (9.3 to 17.9) | 10.1 (7.6 to 12.6) | 7.5 (5.6 to 9.4) | 5.6 (3.8 to 7.3) | 4.1 (2.4 to 5.8) |
| Green | 16.5 (9.6 to 23.4) | 11.7 (8.0 to 15.5) | 8.3 (6.2 to 10.5) | 5.9 (4.4 to 7.5) | 4.2 (2.8 to 5.6) | 3.0 (1.7 to 4.3) |
| Ultraviolet | 6.9 (3.6 to 10.2) | 2.3 (1.4 to 3.3) | 0.8 (0.4 to 1.2) | 0.3 (0.1 to 0.5) | 0.1 (0.0 to 0.2) | 0.0 (0.0 to 0.1) |
| Infrared | 0.0 (0.0 to 0.0) | 0.0 (0.0 to 0.0) | 0.0 (0.0 to 0.0) | 0.0 (0.0 to 0.0) | 0.0 (0.0 to 0.0) | 0.0 (0.0 to 0.0) |
Format: marginal mean (95% confidence interval)
Capillary count per image by fitzpatrick skin type, comparing 4 different-coloured led capillary microscopes. shading indicates 95% confidence intervals around estimates.
The main finding of this study is that capillary density falls with increasing skin type. The very low capillary count in healthy individuals with darker skins means that a clinician without a full understanding of the effect of skin tone may mis-interpret low capillary count (decreased by a factor of 4 to 5) as disease-associated, for example associated with systemic sclerosis, which is always a concern with capillary counts as low as 3 per image frame.
Contrary to expectations, the hypothesis was not proven; cameras with white and green LEDs enabled significantly higher capillary counts in the same participants than in those with infrared and ultraviolet LEDs.
Further work around improvement of capillaroscopy in darker skin tones is required to optimise the technique for individuals with darker skins, potentially alternative illumination colours or post processing of images.
Until we can better visualise capillaries in darker skins, skin tone must be taken into account when interpreting images clinically, particularly when considering capillary count or density.
REFERENCES: NIL .
Acknowledgements: NIL.
Disclosure of Interests: Matthew Parkes: None declared , Stella Nguiffo Nkouontchie: None declared , Lisa Robogo: None declared , Lily Tilson: None declared , Michael Berks: None declared , Graham Dinsdale: None declared , Joanne Manning: None declared , Sarah Wilkinson: None declared , Sarah Groves: None declared , Andy Vail: None declared , Christopher Wagstaff: None declared , Chris Taylor: None declared , Ariane L. Herrick Janssen, AbbVie, Arena, Boehringer Ingelheim, Camurus, Galderma, Gesynta Pharma and Janssen, Gesynta Pharma, Andrea Murray Actelion, Arena and Gesynta Pharma, Actelion.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (