fetching data ... 
Background: Routine Assessment of Patient Index Data 3 (RAPID3) is a simple and efficient patient-reported outcome measure used to assess overall rheumatoid arthritis (RA) activity. It can be easily performed remotely using digital tools, without the need for in-person consultation with a rheumatologist. However, there is an ongoing discussion about how sufficient patient-reported outcomes capture objective inflammatory signs [1, 2].
Objectives: To examine the longitudinal associations between RAPID3 scores across different gender and age groups in RA patients who have been using a smartphone-based symptom diary for remote disease monitoring.
Methods: This is a secondary analysis of real-world data obtained from patients with a clinical diagnosis of RA who attended appointments between 2018 and 2022 and agreed to use a smartphone-based symptom diary, Living With , for remote disease monitoring. The diary was developed with the involvement of patients in its design and production. Patients were asked to report their disease activity weekly by completing the RAPID3 questionnaire. Data analysis included patients with more than two consecutive RAPID3 responses over a 12-month follow-up period. RAPID3 scores were assessed at months 1, 3, 6, 9, and 12. Associations between RAPID3 score, gender, and age were tested using an adjusted multilevel mixed-effects linear regression model. Disease activity categories were defined according to validated thresholds for baseline RAPID3 score [3]. Statistical tests were performed using Stata16.1 (StataCorp, USA). A p-value of <0.05 was used to define associations that were unlikely to have occurred by chance.
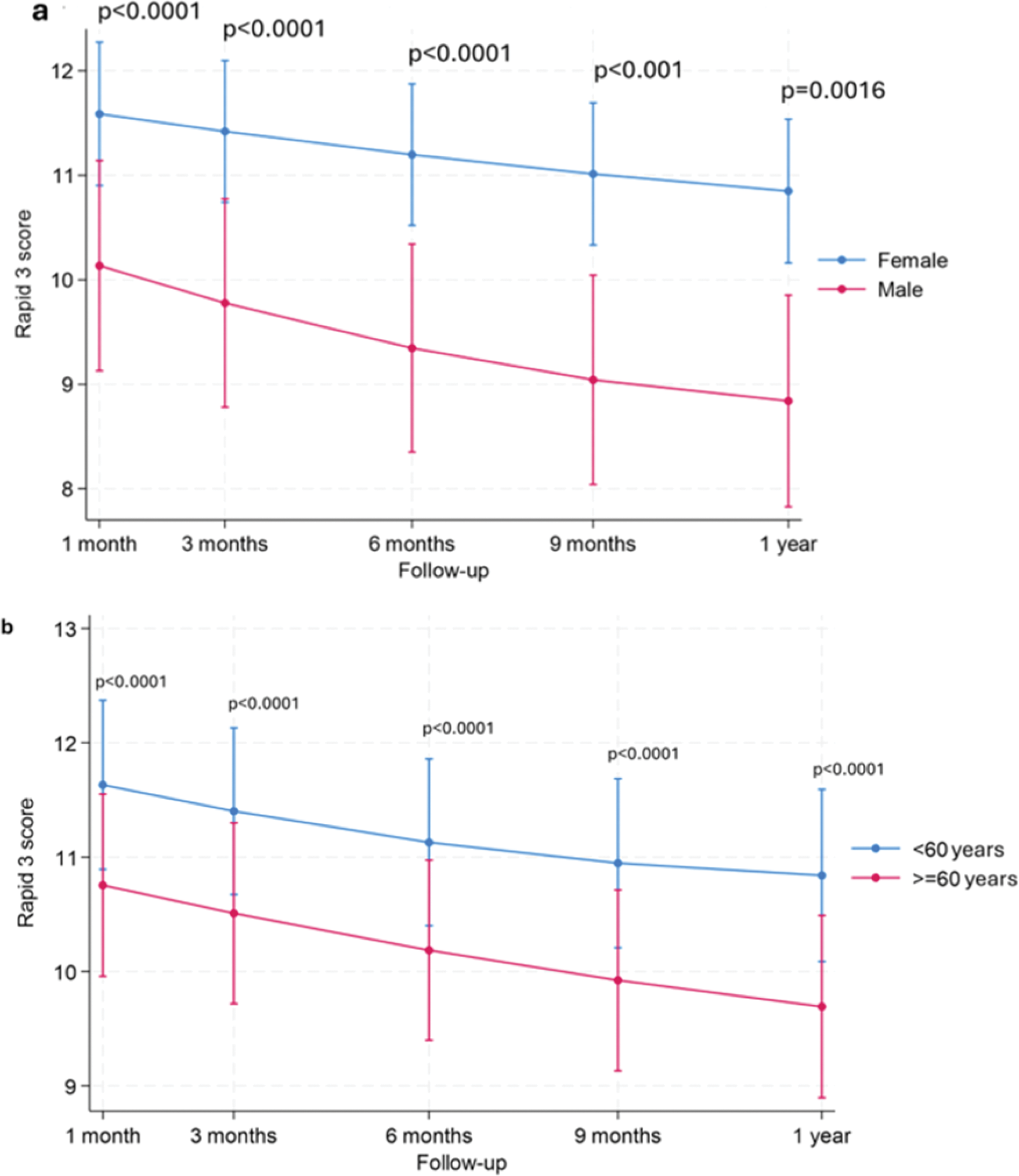
Results: In total, 403 RA patients registered for remote disease monitoring, of whom 79.2% were female with a mean age of 55.5±14.0 years at baseline. Among these, 230 (57.1%) were aged <60 years. Of the total, 367 (91.1%) reported RAPID3 at least once. Of these, 321 (79.7%) completed two consecutive RAPID3 responses during the follow-up period. However, only 149 (40%) of enrolled RA patients completed the full 12-month follow-up. Regarding baseline patient-reported disease activity, 44.7% of enrolled patients reported high disease activity, 22.3% had moderate disease activity, 10.9% had low disease activity, and 13.2% were in remission. In an adjusted multilevel mixed-effects linear regression model, accounting gender and baseline RAPID3 activity, female patients reported significantly higher levels of RAPID3 - disease activity compared to male RA patients at each defined time point (p<0.001). Additionally, in our RA cohort, patients aged <60 years old reported more active disease over time compared to the ≥ 60-year-old group (p<0.0001) (Figure 1).
Conclusion: This analysis highlights novel findings about how the impact and lived experience of RA differ between genders and age groups. The findings reveal that female patients consistently reported higher disease activity levels compared to male patients, potentially due to a variety of factors, including hormonal differences, immune system responses, genetics, and pain perception. Patients under 60 years old reported more active disease over time and causes for this warrant further investigation. These insights emphasize the importance of ongoing monitoring and personalised care strategies, particularly for younger and female RA patients.
Longitudinal RAPID3 scores in RA patients (a) by gender and (b) by age group.
REFERENCES: [1] Boone NW, et al. (2019) Routine Assessment of Patient Index Data 3 (RAPID3) alone is insufficient to monitor disease activity in rheumatoid arthritis in clinical practice. RMD Open; 5.
[2] Ferreira RJO et al. (2019) Dual target strategy: A proposal to mitigate the risk of overtreatment and enhance patient satisfaction in rheumatoid arthritis. Ann Rheum Dis; 78.
[3] Pincus T, Yazici Y, Bergman MJ. (2009) RAPID3, an Index to Assess and Monitor Patients with Rheumatoid Arthritis, Without Formal Joint Counts: Similar Results to DAS28 and CDAI in Clinical Trials and Clinical Care. Rheumatic Disease Clinics of North America; 35.
Acknowledgements: NIL.
Disclosure of Interests: Iuliia Biliavska: None declared, Erik Lenguerrand: None declared, Jon Tobias: None declared, Philip Hamann I have options and a limited royalty agreement with Living With Ltd Software Company for the development of the smartphone application -Living With Rheumatoid Arthritis. In the past three years have also received honoraria from Gilead and AbbVie Pharmaceuticals for the production of training materials on remote monitoring for patients with arthritis.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (