fetching data ... 
Background: Ankylosing Spondylitis (AS) is a chronic inflammatory disease primarily characterized by sacroiliitis and/or spondylitis, often presenting as persistent buttock or back pain [1, 2]. Over time, AS can lead to significant loss of spinal and chest mobility, frequently accompanied by impaired paraspinal muscle function [3]. These muscle changes have been implicated in radiological progression and are increasingly recognized as contributing factors to pain, spinal sagittal imbalance, deformity, and reduced quality of life [4]. While core strength and physical exercise have been shown to improve disease activity and flexibility in AS, the underlying changes in paraspinal muscles and their relationship with disease activity remain poorly understood [5].
Objectives: This study aims to assess functional changes in the paraspinal muscles across cervical, thoracic, and lumbar regions in AS patients, and to correlate surface electromyography (sEMG) data with clinical parameters, including C-reactive protein (CRP) and Erythrocyte Sedimentation Rate (ESR). By exploring these relationships, our study seeks to enhance the understanding of disease activity and contribute to improved diagnosis and rehabilitation strategies for AS.
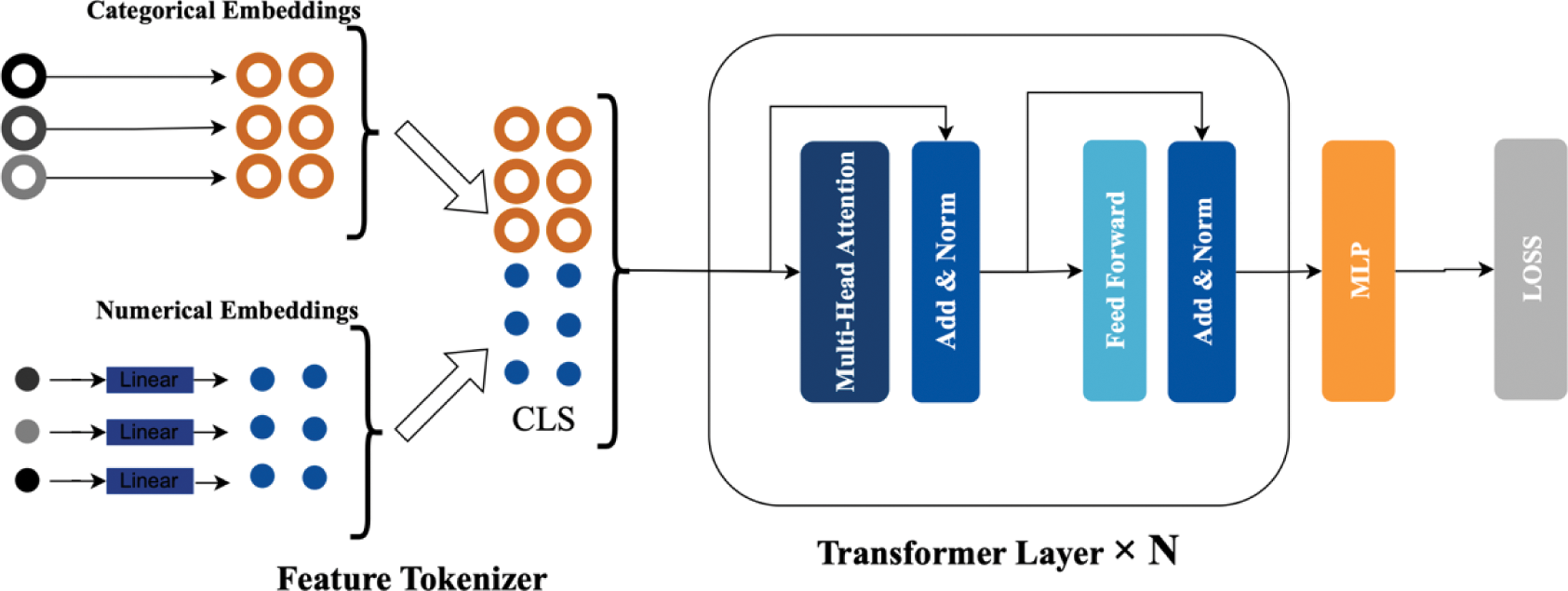
Methods: A cross-sectional study was conducted involving 72 AS patients (mean age: 36.4 years; 53 male, 19 female; mean symptom duration: 7.6 years). Participants performed maximum voluntary contraction of the cervical, thoracic, and lumbar paraspinal muscles. sEMG signals were acquired using a custom-built, non-invasive 8-channel EMG detection system. Key sEMG parameters—including root mean square (RMS), slope sign changes (SSC), median frequency (MF), waveform length (WL), and entropy were computed and compared to healthy controls. The Ankylosing Spondylitis Disease Activity Score (ASDAS) [6] using CRP was correlated with sEMG data. For classification, a tabular dataset comprising the sEMG parameters and ASDAS was analyzed using a deep learning model (FT-Transformer, as illustrated in Figure 1) and three tree-based ensemble methods (CatBoost, XGBoost, and LightGBM). Model performance was evaluated using accuracy, precision, recall, and F1-score.
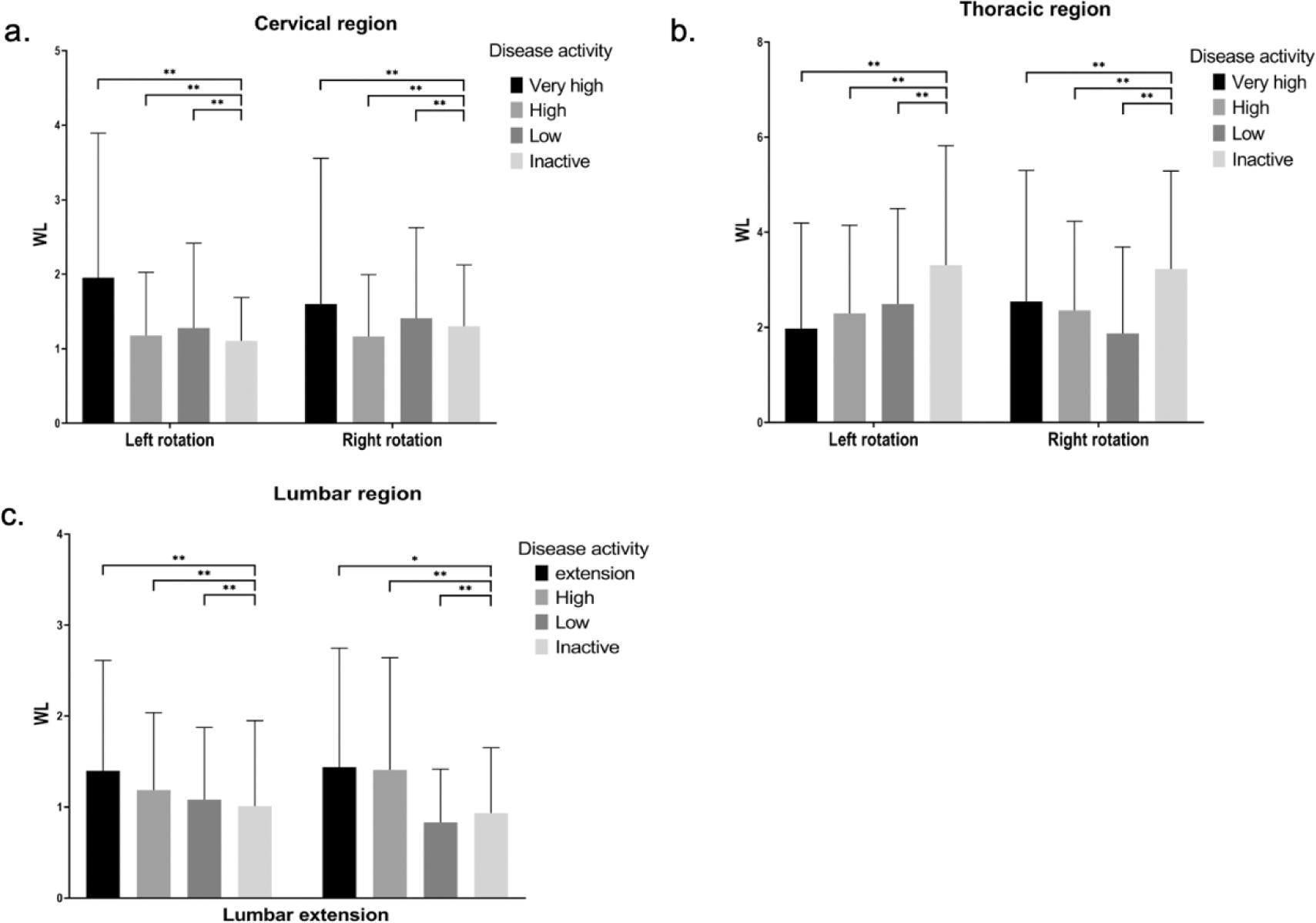
Results: The WL of sEMG signals demonstrate significant variations across different levels of disease activity in AS patients (Figure 2). Notably, the other sEMG characteristics also vary across the cervical, thoracic, and lumbar regions, with pronounced alterations in patients with very high level of disease activity. These findings indicate a strong association between increased disease activity and reduced paraspinal muscle function across all spinal regions. Among the machine learning models tested, the FT-Transformer demonstrates superior performance, achieving an accuracy of 74.58%, a precision of 73.80%, a recall of 79.32%, and an F1-score of 75.84%, outperforming the tree-based ensemble methods.
Conclusion: This study demonstrates that sEMG characteristics of paraspinal muscles are significantly correlated with disease activity in patients with AS. The use of non-invasive sEMG provides a quantitative and reliable method for assessing muscle conditions, enhancing the accuracy of disease activity evaluations, and potentially informing clinical guidelines. Furthermore, machine learning models such as FT-Transformer offer promising tools for classifying disease activity. These findings underscore the potential of sEMG and advanced analytics in supporting personalized diagnosis and optimizing rehabilitation strategies for AS patients.
REFERENCES: [1] Mauro, D. et al. Ankylosing spondylitis: an autoimmune or autoinflammatory disease? Nat. Rev. Rheumatol. 17, 387–404 (2021).
[2] McGonagle, D., David, P., Macleod, T. & Watad, A. Predominant ligament-centric soft-tissue involvement differentiates axial psoriatic arthritis from ankylosing spondylitis. Nat. Rev. Rheumatol. 19, 818–827 (2023).
[3] Seres, I. G. et al. 732 The relationship between myotonometry parameters and spinal mobility in ankylosing spondylitis patients included in a physical exercise program. Balneo PRM Res. J. 15, 732–732 (2024).
[4] Sarac, D. C. et al. Association of Core Muscle Endurance Times With Balance, Fatigue, Physical Activity Level, and Kyphosis Angle in Patients With Ankylosing Spondylitis. JCR J. Clin. Rheumatol. 28, e135 (2022).
[5] De Mits, S. et al. Maximal Exercise Tolerance, Objective Trunk Strength, and Mobility Measurements in Axial Spondyloarthritis. J. Rheumatol. jrheum.2023-1046 (2024) doi:10.3899/jrheum.2023-1046.
[6] Machado, P. et al. Ankylosing Spondylitis Disease Activity Score (ASDAS): defining cut-off values for disease activity states and improvement scores. Ann. Rheum. Dis. 70, 47–53 (2011).
The whole structure of FT-Transformer
Comparison of WL across different disease activity levels in AS patients: (a) cervical region during left and right neck rotation, (b) thoracic region during left and right chest rotation, and (c) lumbar region during lumbar extension. *P<0.05. **P<0.03.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (