fetching data ... 
Background: Interstitial lung disease (ILD) is diagnosed by chest high-resolution computed tomography (lung HR-CT) and the role of lung ultrasound (LUS) is still being discussed. Despite several studies in this years showing the performance of LUS to detect ILD, LUS was not mentioned in the 2023 ACR/CHEST Guideline for the Screening and Monitoring of ILD in people with Systemic Autoimmune Rheumatic Diseases [1].
Objectives: This study aims to evaluate the LUS capacity to discriminate different ILD patterns in patients with rheumatic diseases, such as Ground Glass (GG), Honeycombing (HC) and mixed pattern (HC + GG). Another objective is to evaluate the possible relationship between the number of B-lines and the volume of extension of the main lesions in the HRTC assessed by artificial intelligence (AI).
Methods: Eighty patients with Rheumatic diseases (54 with SSc, 7 AR, 4 overlap SSc/AR, 3 SSc/SS, 2 AR/SS, 2 EGPA, 2 UCTD, 2 SS, 1 Antisynthetase syndrome, 1 AR/LES, 1 PsA, 1 MCTD) were recruited for this study, followed by Rheumatology Unit of Policlinico of Foggia. All patients satisfied their respective classification criteria and age older than 18 years. HRTC performed within six months before or six months after LUS evaluation; and availability of recent and complete pulmonary function test with FVC and DLCO. We excluded patients with BPCO, lung cancer, recent lung infection, heart failure, pulmonary oedema, PAH, thoracic surgery and radiotherapy.
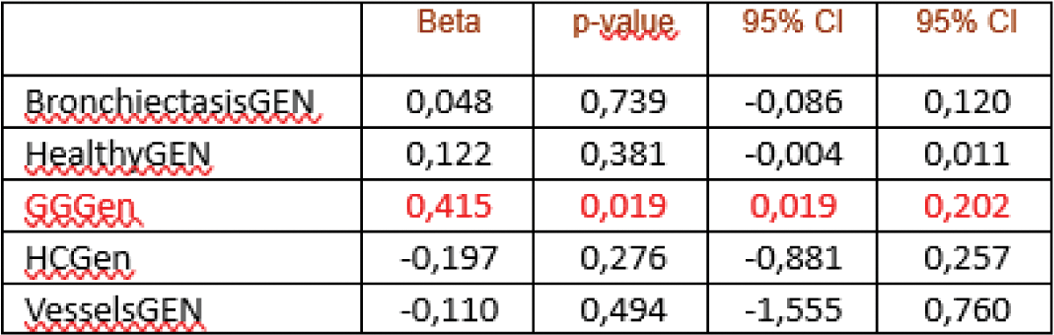
Results: ILD was observed in 50 (62.5%) patients (35 with GG pattern, 7 HC and 8 HC + GG). By ROC curve analysis, higher accuracy (0.63), sensitivity (91.4%), and specificity (36.6%) were found for B-lines (p=0,039) to detect GG and for pleural line thickness (accuracy 0.86, sensitivity 100%, specificity 72.2% p=0.001) and subpleural cyst (accuracy 0.76, sensitivity 62.5%, specificity 90.3%, p=0.015) to detect HC + GG pattern. The best performance among LUS signs for HC patterns was observed for pleural line irregularity (accuracy 0.68, sensitivity 100%, specificity 37%, p=0.108). By linear regression analysis, we evaluated the number of B-lines and the volume of extension of the main lesions in the HRTC assessed by AI that results positively associated (beta 0.415, 95% CI 0.019 – 0.202, p=0.019).
Conclusion: Our study demonstrated that the LUS presented a high capacity to discriminate the different patterns of ILD in rheumatic disease. Therefore, the hypothesis of using transthoracic LUS as a screening method for the evaluation of the presence of ILD and to establish the correct timing for the execution of chest HR-CT, in order to avoid patients from excessive exposure to ionising radiation is supported. Further clinical studies, on a larger cohort of patients, confirming these results are needed to support these hypotheses and standardize the method. For the first time, we demonstrate a positive association between the number of B-line and the extension of GG assessed by HR chest CT with the help of AI.
REFERENCES: [1] Johnson, Sindhu R et al. “2023 American College of Rheumatology (ACR)/American College of Chest Physicians (CHEST) Guideline for the Screening and Monitoring of Interstitial Lung Disease in People with Systemic Autoimmune Rheumatic Diseases.” Arthritis & rheumatology (Hoboken, N.J.) vol. 76,8 (2024): 1201-1213. doi:10.1002/art.42860.
Table 1.
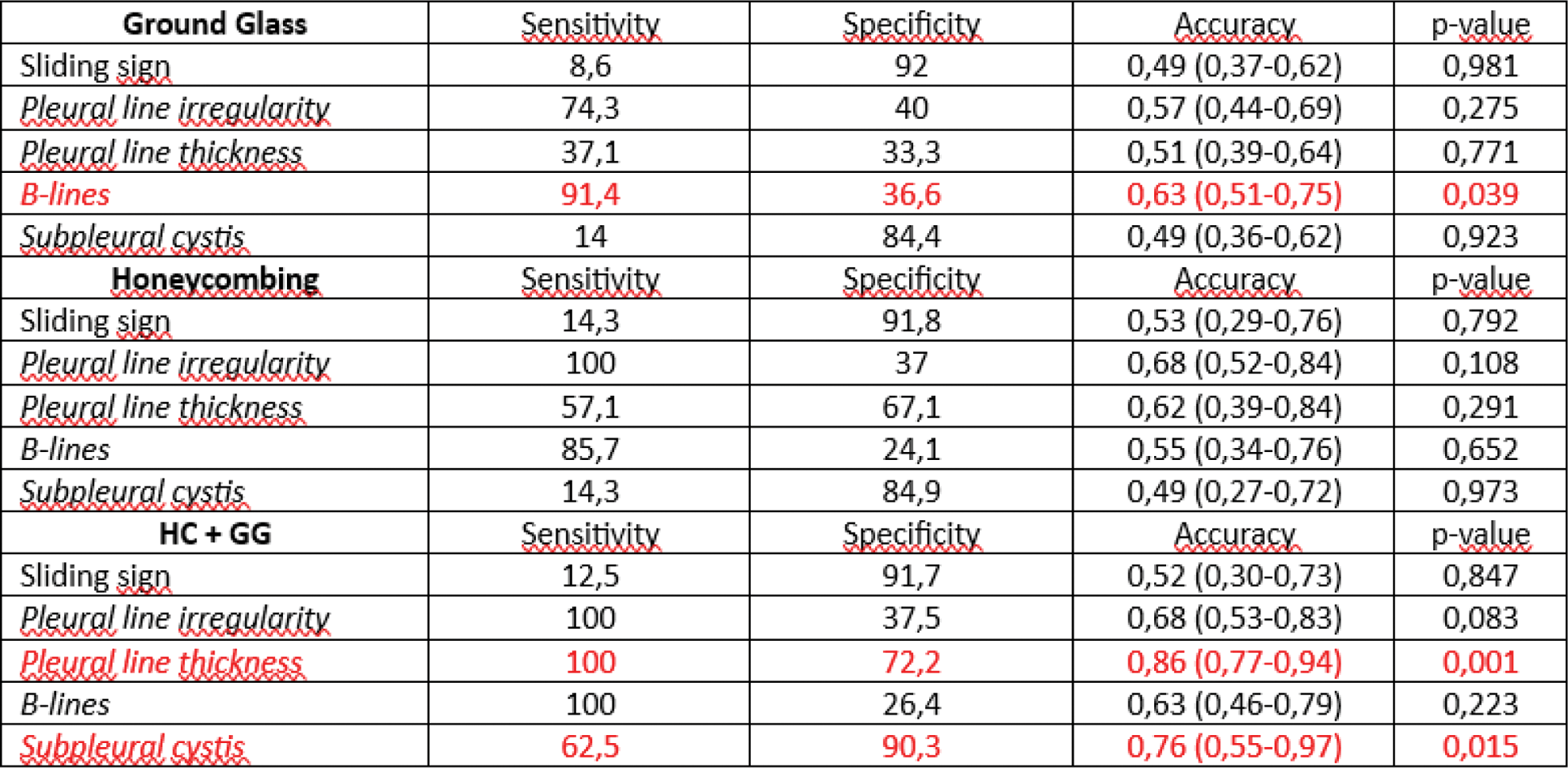
Table 2.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (