fetching data ... 
Background: IgG4-related disease (IgG4-RD) is a fibro-inflammatory disorder characterized by dense lymphoplasmacytic infiltration and IgG4-positive plasma cells within affected tissues. While cardiovascular involvement in IgG4-RD is rare, coronary artery stenosis as an isolated presentation is exceptionally uncommon.
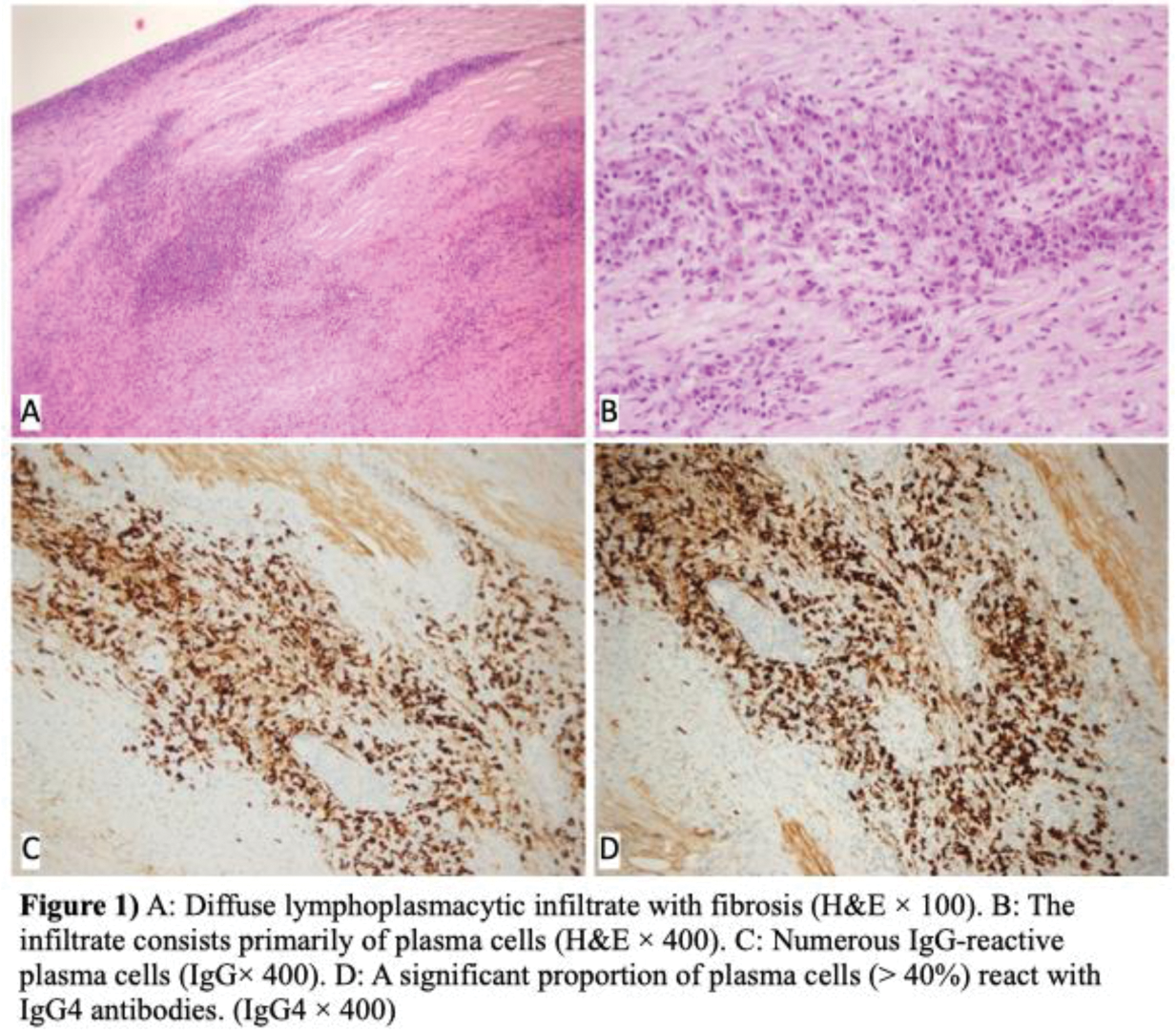
Case presentation: A 27-year-old male presented with acute myocardial infarction in January 2023. Coronary angiography (CAG) revealed 30% stenosis in the distal left main coronary artery (LMCA), 99% stenosis in the proximal left anterior descending artery (LAD), 80% stenosis in the osteal circumflex artery (CX), and 80% stenosis in the distal right coronary artery. Primary percutaneous coronary intervention was performed on the LAD, achieving full revascularization. Notably, the patient had no significant medical history, family history of coronary artery disease, or hyperlipidemia, and lacked conventional cardiovascular risk factors. Despite initial management, the patient developed presyncope and nausea in December 2023. Repeat CAG revealed progression of LMCA stenosis, with 80% distally and 98% in the long osteal segment, and persistent multivessel involvement, necessitating four-vessel coronary artery bypass grafting. Intraoperative findings included diffuse narrowing of coronary arteries and segmental thickening of the ascending aorta. Histopathological examination of the aortic tissue revealed myointimal proliferation, lymphoplasmacytic infiltration across all layers, obliterative vasculopathy, partial storiform fibrosis, and medial elastic fiber loss. Immunohistochemical staining confirmed an IgG4/IgG ratio >40%, leading to a diagnosis of IgG4-related aortitis (Figure 1). Serum IgG4 levels were significantly elevated at 442 mg/dL. The patient received high-dose pulse steroids (500 mg daily), tapered to 5 mg/day, alongside maintenance therapy with rituximab every six months, mycophenolate mofetil, and standard cardiovascular medications. At the 6-month follow-up, serum IgG4 levels normalized to 97.4 mg/dL. The patient reported no anginal symptoms or other complaints.
Learning points for clinical practice: IgG4-RD, although rare, should be considered a differential diagnosis in young patients with progressive coronary artery stenosis and myocardial ischemia, even in the absence of other systemic manifestations. Early recognition and initiation of targeted immunosuppressive therapy can prevent further vascular damage and improve long-term outcomes.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (