fetching data ... 
Background: RA synovitis is characterized by synovial hyperplasia, increase of the stromal compartment density and infiltration of inflammatory cells whose quantification is associated with disease activity and response to MTX [1]. In our previous study, we identified four subgroups based on routine clinical data, defined primarily by their Joint Involvement Patterns (JIP): JIP-feet, JIP-oligo, JIP-hand and JIP-poly. These subgroups were linked to differences in MTX outcomes after one year across various centers, with JIP-hand showing the best response and JIP-poly the worst [2].
Objectives: In this study we aimed to dissect whether different phenotypic clinical features might correlate with differences in synovial tissue histological composition.
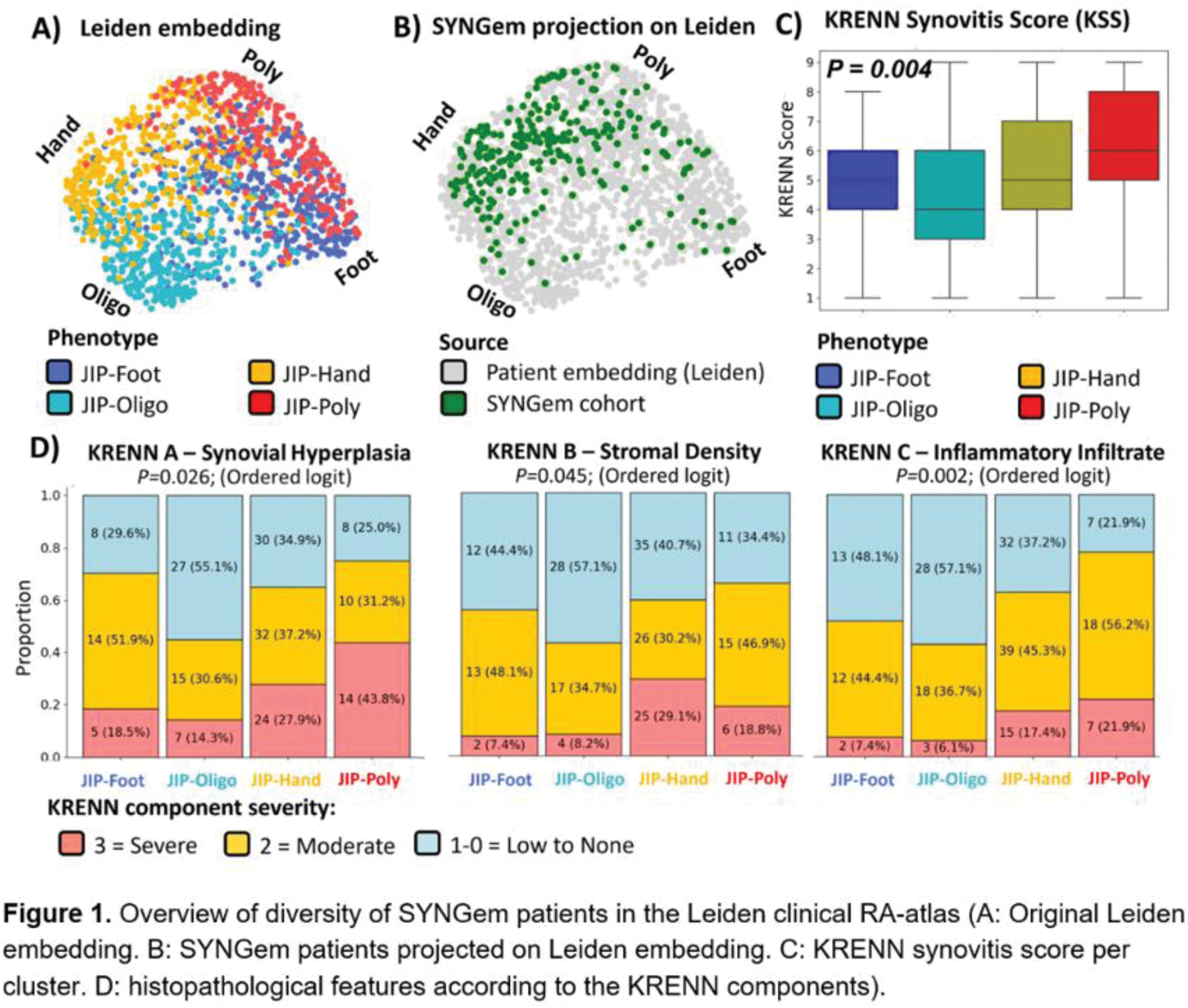
Methods: 262 csDMARD naive RA patients of the SYNGem cohort (Rome-Italy) were included in the analysis [1]. Using baseline clinical information only, we mapped them into the previous embedding and categorized them into the four JIP-phenotypes found in our previous study: JIP-feet, JIP-oligo, JIP-hand and JIP-poly (Figure. 1) [2, 3]. Synovial biopsies were taken from the most inflamed joint, and after hematoxylin-eosin staining, the severity of synovitis was graded using the Krenn synovitis score (KSS) [4] according to the three synovial membrane features (synovial lining cell layer, stromal cell density and inflammatory infiltrate), each ranked on a scale from none (0), slight (1), moderate (2), and severe (3). To avoid bias from biopsy location, we studied only the knee joint biopsies (n=194). We used an ordered logistic regression to identify differences in histopathological features between the clusters. Since the lowest level ‘none’ was highly underrepresented (or even absent in some groups), we combined it with the ‘low’ level [1]. Next, we used Wald post-hoc tests to compare the log-odds of group categories to ascertain the biggest local differences.
Results: All of the four phenotypes were present in the SYNGem dataset (Table 1 & Figure. 1B), with the JIP-hand phenotype being the most prevalent. The KSS scores revealed a clear overall trend in synovitis severity across the subgroups ( P= 0.004; Figure 1C). The JIP-poly subgroup exhibited the highest levels of synovitis, followed by moderate levels in the JIP-feet and JIP-hand subgroups, while the JIP-oligo subgroup showed the lowest levels of synovitis. The clusters showed histopathological variations across the three components (i: P= 0.026, ii: P=0.045 , iii: P= 0.002; Figure 1D). These differences were primarily driven by the large distinction between the more stereotypical RA clusters (hand and poly) versus the oligoarthritic group. In particular, the JIP-oligo had a low-grade synovitis level in the majority of patients. Conversely, the JIP-poly showed a severely hyperplastic synovial lining (>5 layers) in 44% of patients and a severe sublining inflammatory infiltration in 22% of patients, both significantly higher compared to the JIP-oligo (14%, P=0.002 and 6%, P=0.001, respectively).The JIP-hand dominated pattern also corresponded to a higher synovial hyperplasia and leukocyte infiltration than the JIP-oligo clusters ( P =0.015; P =0.013). Furthermore, 29.1% of patients with the JIP-hand phenotype exhibited severe stromal cell proliferation, along with pannus formation compared to only 7.4% of patients with the JIP-feet and 8.2% with JIP-oligo phenotype ( P =0.211, P =0.013). For the JIP-feet phenotype, there was no specific category where it stood out in terms of synovitis severity, showing average scores across all severity components. Since disease activity is associated with histopathological synovitis severity, we performed an additional analysis where we adjusted for disease activity, to ensure that the cluster effect did not simply reflect the DAS-categories. The results showed that significance persisted for synovial hyperplasia ( P =0.035) and inflammatory infiltrate ( P =0.005) but not for stromal density ( P =0.082).
Conclusion: Our findings revealed differences in the synovitis degree across clinically-defined JIP subgroups. Both JIP-hand and JIP-poly exhibited the highest levels of synovitis, with JIP-poly showing more lining hyperplasia and sublining leukocytic infiltration, while JIP-hand had higher stromal density. Whereas, JIP-feet showed a moderate degree and JIP-oligo had a low-grade synovitis. Further research is needed to determine if JIP subgroups, informing on synovial histological features, can be linked to first-line MTX response as previously demonstrated.
Cluster table for SYNGem cohort. The clinical variables used for clustering are marked with the gamma symbol (ɣ).
| Total | JIP-Foot | JIP-Oligo | JIP-Hand | JIP-Poly | |
|---|---|---|---|---|---|
| N | 194 | 27 | 49 | 86 | 32 |
| Sex, female ɣ [n(%)] | 150 (77.3) | 18 (66.7) | 41 (83.7) | 66 (76.7) | 25 (78.1) |
| Age ɣ (SD, yr ) | 56.1 (14.9) | 52.9 (14.0) | 51.1 (14.6) | 62.1 (12.8) | 50.4 (15.1) |
| KSS | 5 (4-7) | 5 (4-6) | 4 (3-6) | 5 (4-7) | 6 (5-8) |
| RF ɣ [n(%] | 83 (42.8) | 8 (29.6) | 24 (49.0) | 39 (45.3) | 12 (37.5) |
| ACPA ɣ [n(%)] | 91 (46.9) | 11 (40.7) | 23 (46.9) | 40 (46.5) | 17 (53.1) |
| ESR ɣ (IQR, mm/hr ) | 43 (20-64) | 33 (16-52) | 32 (14-53) | 50 (24-77) | 52 (30-66) |
| SJC (IQR ) | 10 (7-12) | 11 (8-12) | 4 (4-6) | 10 (8-13) | 14 (10-20) |
| TJC (IQR ) | 13 (9-16) | 14 (12-16) | 8 (6-10) | 14 (12-16) | 19 (14-23) |
| DAS28 (IQR ) | 5.5 (4.8-6.7) | 5.7 (5.1-6.2) | 4.6 (4.1-5.2) | 5.8 (5.0-6.8) | 6.9 (6.2-7.9) |
REFERENCES: [1] Alivernini S, Tolusso B, Gessi M, et al. Inclusion of Synovial Tissue-Derived Characteristics in a Nomogram for the Prediction of Treatment Response in Treatment-Naive Rheumatoid Arthritis Patients. Arthritis Rheumatol. 2021 Sep;73(9):1601-1613. DOI: 10.1002/art.41726.
[2] Maarseveen, T et al. DOI: 10.1101/2023.09.19.23295482.
[3] Leiden patient embedding. Rheumalyze.
[4] Krenn V, et al. DOI: 10.1111/j.1365-2559.2006.02508.x.
Acknowledgements: This project has received funding from Horizon Europe programme under grant agreement no. 101095052 (SQUEEZE), no. 101080711 (SPIDERR), ZonMW klinische fellow no. 40-00703-97-19069, and ZonMw Open Competitie 2021 no. 09120012110075.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (