EXPLORING THE GENETIC BASIS OF CLINICAL HETEROGENEITY IN GIANT CELL ARTERITIS
Keywords: -omics, Rare/orphan diseases, Epitranscriptomics, Epigenetics, And genetics
G. Borrego-Yaniz1, V. Fuentes-Moreno1, J. Hernández-Rodríguez2, A. Vaglio3,4, S. Castañeda5, R. Solans-Laqué6, N. Khalidi7, C. Langford8, S. R. Ytterberg9, L. Beretta10, M. Govoni11, G. Emmi12,13, M. A. Cimmino14, T. Witte15, T. Neumann16,17, J. Holle18, V. Schönau19, G. Pugnet20, [. Papo]21, J. Haroche22, A. Mahr23, L. Mouthon24, Ø. Molberg25, A. Diamantopoulos26, A. Voskuyl27, T. Daikeler28, C. Berger29, E. Molloy30, D. Blockmans31, Y. van Sleen32, S. GCA Group33, U. G. Consortium34, V. C. Research Consortium35, N. Ortego-Centeno36, E. Brouwer32, P. Lamprecht37, S. Klapa37, C. Salvarani38, P. Merkel39, M. C. Cid2, M. Á. González-Gay40,41, A. Morgan42, J. Martin1, A. Márquez1
1Institute of Parasitology and Biomedicine López-Neyra, CSIC, Granada, Spain
2Hospital Clinic of Barcelona, University of Barcelona, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Vasculitis Research Unit, Department of Autoimmune Diseases, Barcelona, Spain
3University of Florence, Department of Biomedical Experimental and Clinical Sciences “Mario Serio”, Florence, Italy
4Meyer Children’s Hospital, Nephrology and Dialysis Unit, Florence, Italy
5Hospital de la Princesa, IIS-IP, Department of Rheumatology, Madrid, Spain
6Hospital Vall d’Hebron, Autonomous University of Barcelona, Autoimmune Systemic Diseases Unit, Department of Internal Medicine, Barcelona, Spain
7McMaster University, Division of Rheumatology, Hamilton, Canada
8Cleveland Clinic, Department of Rheumatic and Immunologic Diseases, Cleveland, United States of America
9Mayo Clinic, Division of Rheumatology, Rochester, United States of America
10Referral Center for Systemic Autoimmune Diseases, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico di Milano, Milan, Italy
11Azienda Ospedaliero Universitaria S. Anna, University of Ferrara, Department of Rheumatology, Ferrara, Italy
12University of Trieste, Department of Medical, Surgery and Health Sciences, Trieste, Italy
13Centre for Inflammatory Diseases, Monash Medical Centre, Monash University, Department of Medicine, Clayton, Australia
14University of Genova, Research Laboratory and Academic Division of Clinical Rheumatology, Department of Internal Medicine, Genova, Italy
15Hannover Medical School, Hannover, Germany
16Klinik für Innere Medizin III, University-Hospital Jena, Jena, Germany
17Cantonal Hospital St. Gallen, Department of Rheumatology, St. Gallen, Switzerland
18Vasculitis Clinic, Klinikum Bad Bramstedt & University Hospital of Schleswig Holstein, Bad Bramstedt, Germany
19Friedrich-Alexander-Universität Erlangen-Nürnberg and Uniklinikum Erlangen, Department of Medicine 3 - Rheumatology and Immunology, Erlangen, Germany
20Toulouse University Hospital Center, Department of Internal Medicine, Tolouse, France
21Hôpital Bichat, Université Paris-Cité, Service de Médecine Interne, Paris, France
22Assistance Publique-Hôpitaux de Paris (AP-HP), Pitié-Salpêtrière Hospital & French Reference Center for Rare Auto-Immune & Systemic Diseases, Department of Internal Medicine, Paris, France
23Centre of Research in Epidemiology and Statistics, Sorbonne Paris Cité Research Center UMR 1153, ECSTRRA Research Unit, Paris, France
24Cochin Hospital, National Referral Center for Rare Systemic Autoimmune and Autoinflammatory Diseases of the Ile de France, East and West, AP-HP, Université Paris Cité, Internal Medicine Department, Paris, France
25Oslo University Hospital, Department of Rheumatology, Oslo, Norway
26Hospital of Southern Norway Trust, Department of Rheumatology, Kristiansand, Norway
27Amsterdam UMC, Department of Rheumatology and Clinical Immunology, Amsterdam, Netherlands
28University Hospital Basel, Department of Rheumatology and Department of Clinical Research University of Basel, Basel, Switzerland
29University Hospital Basel, Translational Immunology and Medical Outpatient Clinic, Departments of Biomedicine and Internal Medicine, Basel, Switzerland
30Centre for Arthritis and Rheumatic Diseases, St Vincent’s University Hospital, Department of Rheumatology, Dublin, Ireland
31University Hospital Gasthuisberg, Department of General Internal Medicine, Leuven, Belgium
32University of Groningen, University Medical Center Groningen, Department of Rheumatology and Clinical Immunology, Groningen, Netherlands
33-, -, Spain
34-, -, United Kingdom
35-, -, United States of America
36University of Granada, Instituto de Investigación Biosanitaria de Granada ibs.GRANADA, Department of Medicine, Granada, Spain
37University of Lübeck, Department of Rheumatology and Clinical Immunology, Lübeck, Germany
38Azienda USL-IRCCS di Reggio Emilia and Università di Modena e Reggio Emilia, Reggio Emilia, Italy
39University of Pennsylvania, Division of Rheumatology, Department of Medicine, Philadelphia, United States of America
40IIS-Fundación Jiménez Díaz, Division of Rheumatology, Madrid, Spain
41University of Cantabria, Department of Medicine, Santander, Spain
42School of Medicine, University of Leeds and NIHR Leeds Biomedical Research Centre, Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom
Background: Giant cell arteritis (GCA) is a large-vessel vasculitis primarily affecting the aorta and its branches. GCA presents with a wide range of clinical manifestations, reflecting its complex and heterogeneous nature. These disease features include cranial symptoms such as headache, vision abnormalities, and ischemic stroke, as well as the association with polymyalgia rheumatica. This clinical variability complicates diagnosis and management of GCA.
Objectives: The aim of this study was to identify genetic risk factors associated with key clinical manifestations of GCA by testing genome-wide association.
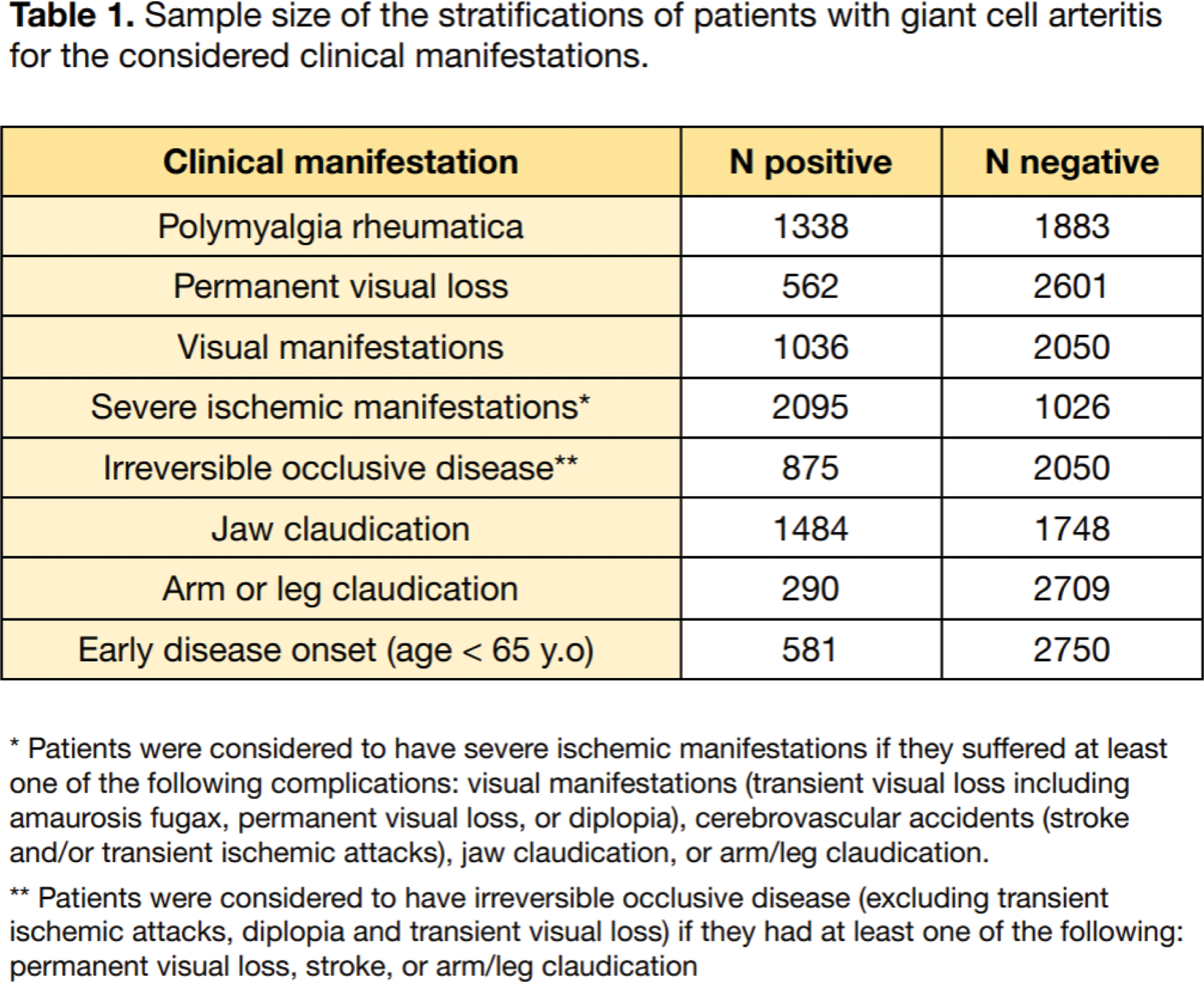
Methods: Genomic data from 3,498 patients with GCA and 15,550 healthy controls from a previous study [1] were analyzed to investigate the genetic background associated with GCA-related manifestations. Patients with GCA were stratified according to the presence/absence of clinical phenotypes (shown in Table 1 along with their respective sample sizes). Three logistic regression analyses were performed for each trait, adjusting for the first 10 principal components and sex as covariates, comparing: i) manifestation-positive patients and unaffected controls, ii) manifestation-negative patients and unaffected controls, and iii) patients with and without the considered manifestation. A signal was considered specifically associated with a clinical phenotype if it reached genome-wide significance (p < 5×10⁻⁸) in the case-control comparison and also nominal significance in intra-case comparisons. The HLA region was excluded from the analysis due to its high linkage disequilibrium and complex genetic architecture. Gene annotation was conducted based on SNP-to-gene distance and functional information, including expression and protein quantitative trait locus (eQTL/pQTL) data from blood and vascular tissues.
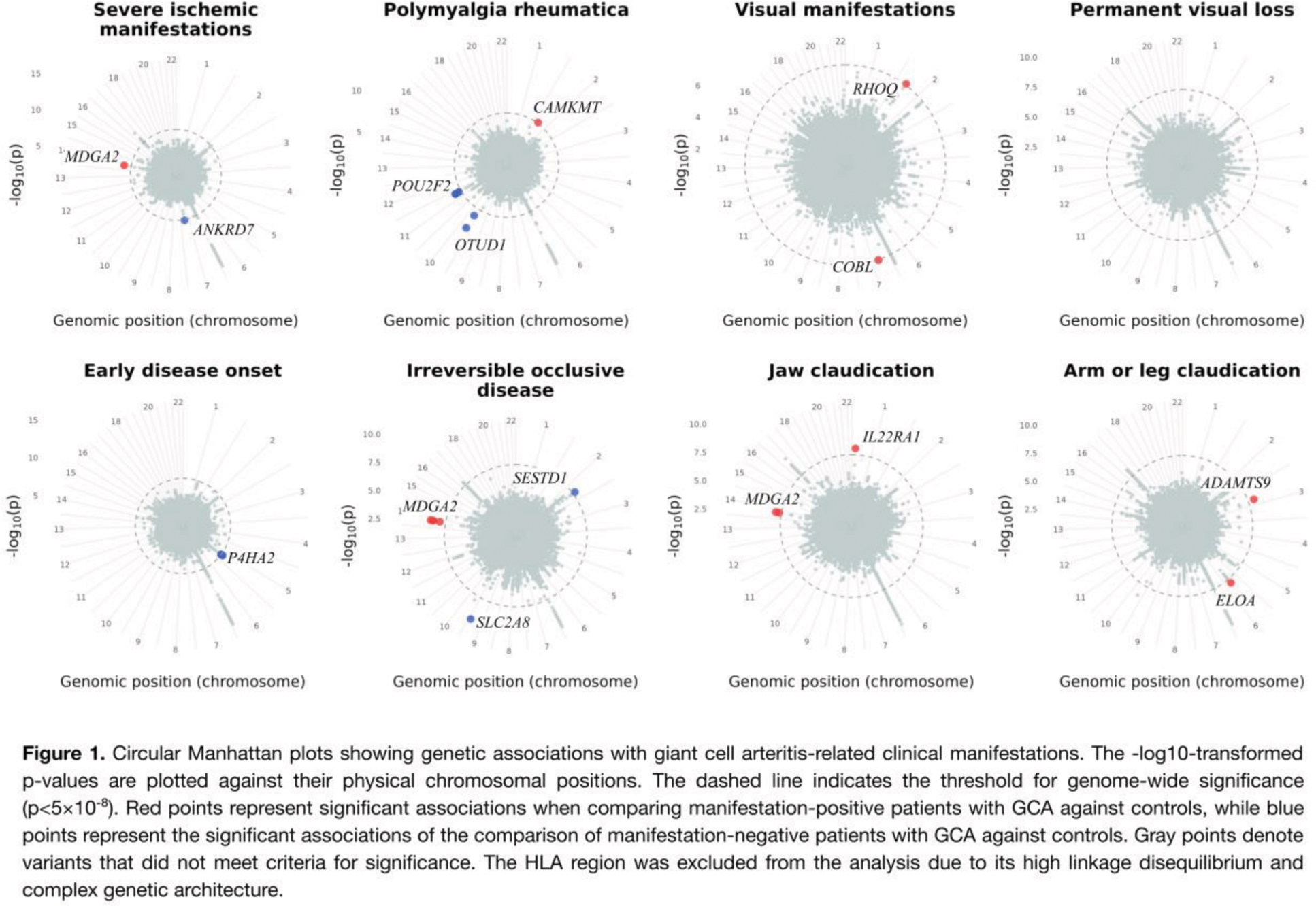
Results: Thirteen non-HLA significant genetic associations across seven distinct GCA-related manifestations were identified: early disease onset, polymyalgia rheumatica, visual manifestations, severe ischemic manifestations, jaw claudication, arm or leg claudication, and irreversible occlusive disease (Figure 1). No significant association was found for permanent visual loss. These loci exhibited notable effect sizes and comprised novel associations for this pathology. Key findings included:
RHOQ
, associated with visual manifestations (rs6746695, p=4.14×10⁻⁸, OR=3.19), which regulates angiogenesis via Notch signaling [2];
IL22RA1
, associated with jaw claudication (rs72663289, p=1.36×10⁻8, OR=3.13), an interleukin receptor that has been described to be upregulated in GCA-affected arteries, as well as peripheral blood mononuclear cells and plasma from patients with GCA [3]; and
OTUD1
, associated with the absence of polymyalgia rheumatica (rs138303599, OR=6.10, p=1.01×10-10), which can promote inflammation and remodeling in cardiac tissue by affecting STAT3 [4, 5]. Additionally, the gene
P4HA2
, previously identified as involved in GCA, was found to be specifically associated with late-onset cases (rs419291, p=2.89×10⁻⁸, OR=1.19).
Conclusion: This study represents the first genome-wide association analysis of GCA-specific manifestations, deepening our understanding of the genetic basis underlying the disease’s clinical heterogeneity. These findings may lead to earlier diagnosis, improved monitoring of disease activity, and more targeted therapeutic strategies for this complex condition.
REFERENCES: [1] Borrego-Yaniz G, Ortiz-Fernández L, Madrid-Paredes A, et al (2024) Risk loci involved in giant cell arteritis susceptibility: a genome-wide association study. Lancet Rheumatol 6:e374–e383.
[2] Bridges E, Sheldon H, Kleibeuker E, et al (2020) RHOQ is induced by DLL4 and regulates angiogenesis by determining the intracellular route of the Notch intracellular domain. Angiogenesis 23:493–513.
[3] Zerbini A, Muratore F, Boiardi L, et al (2018) Increased expression of interleukin-22 in patients with giant cell arteritis. Rheumatology (Oxford) 57:64–72.
[4] Wang M, Han X, Yu T, et al (2023) OTUD1 promotes pathological cardiac remodeling and heart failure by targeting STAT3 in cardiomyocytes. Theranostics 13:2263–2280.
[5] Oikawa D, Gi M, Kosako H, et al (2022) OTUD1 deubiquitinase regulates NF-κB- and KEAP1-mediated inflammatory responses and reactive oxygen species-associated cell death pathways. Cell Death Dis 13:694.