fetching data ... 
Background: Early treat-to-target strategies, aiming for a rapid control of disease activity, have proven their benefits on clinical outcomes in rheumatoid arthritis (RA). The choice of the disease modifying antirheumatic drugs (DMARDs) might be relevant given the variability in the time to onset of action between particular drugs. JAK-inhibitors (JAKi) are a targeted synthetic DMARD (tsDMARD) and have demonstrated a rapid onset of action. However, it is unclear how they compare to other DMARDs and whether adding glucocorticoid (GC) as co-medication is a determinant factor in achieving a prompt response.
Objectives: This study aims to assess and compare short-term (3-month) effectiveness of JAKi and biologic DMARDs (bDMARDs), in relation to concomitant GC use, in a real-world RA cohort from an international collaboration of registers (“JAK-pot” collaboration).
Methods: Study participants include RA patients of 12 national registers initiating either JAKi, TNF-inhibitors (TNFi), IL-6 inhibitors (IL-6i) or abatacept (ABA) during the period when JAKi became available. Baseline characteristics were compared between treatments using ANOVA or Kruskal-Wallis tests for continuous variables and Chi-square tests for categorical variables. Treatment effectiveness was assessed by comparing CDAI trajectories for each treatment using polynomial mixed model on all recorded visits and in a subpopulation of patients with concomitant use of GC. Analyses were adjusted for age, gender, seropositivity, smoking status, BMI ≥30kg/m 2 , disease duration, number of previous b/tsDMARD, glucocorticoid treatment (in the full population), and concomitant treatment (csDMARD).
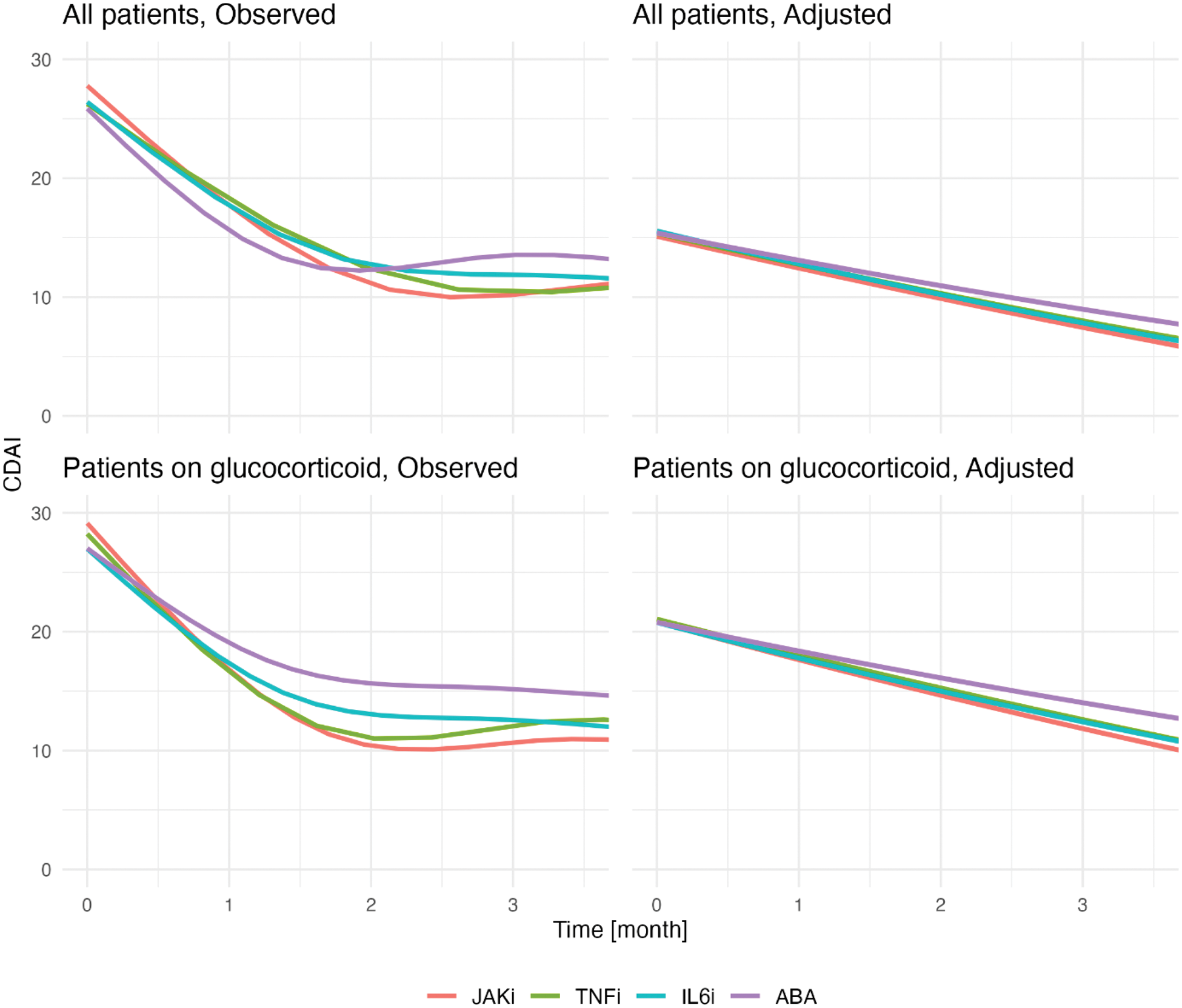
Results: A total of 9,544 patients (28,142 visits, of which 14,129 with concomitant GC) were included (3291 JAKi, 4289 TNFi, 1315 IL6i, 649 ABA). About half of the patients (47.4%) were receiving concomitant GC therapy at ts/bDMARD initiation. The proportion of GC use was lower in patients receiving TNFi (p<0.001). They were also significantly younger with shorter disease duration and less frequent previous b/tsDMARDs than the other groups at baseline. Patients receiving JAKi had the longest disease duration, and a higher baseline CDAI (Table 1). In the observed trajectories, CDAI improved quickly during the first 2 months of treatment (Figure 1, top left), with a sharper decrease for JAKi and TNFi. In adjusted analyses, the decrease was largest for JAKi (slope: -0.22 month), and lower for the other DMARDs, though the difference only reached significance for TNFi (TNFi -0.20/month, change in slope: +0.02, p<0.001). In the subpopulation with concomitant use of GC, adjusted trajectories analysis showed that CDAI improvement rates were slightly stronger for all DMARDs. This larger decrease in CDAI was more pronounced in patients receiving JAKi (-0.26/month, p<0.001) compared to other bDMARDs (TNFi -0.24/month, IL6i -0.22/month, ABA 0.21/month, changes in slope: TNFi +0.02, IL6i +0.04, ABA +0.05, p-values < 0.05).
Baseline characteristics.
| JAK inhibitors | TNF inhibitors | IL6 inhibitors | Abatacept | p | |
|---|---|---|---|---|---|
| N = | 3291 | 4289 | 1315 | 649 | |
| Age, years | 57.8 [49.6, 66.0] | 56.0 [46.3, 64.6] | 59.0 [50.6, 66.8] | 61.6 [53.8, 70.7] | <0.001 |
| Female sex (%) | 2727 (82.9) | 3424 (79.8) | 1059 (80.6) | 506 (78.0) | 0.002 |
| Current smoker (%) | 244 (18.7) | 478 (21.8) | 163 (20.4) | 75 (19.7) | 0.169 |
| BMI, kg/m 2 | 25.7 [22.7, 29.8] | 25.9 [22.9, 30.1] | 25.9 [22.9, 29.6] | 26.0 [22.8, 29.9] | 0.293 |
| Disease duration, years | 11.6 [5.9, 19.2] | 7.8 [3.4, 14.7] | 10.4 [5.0, 18.1] | 9.8 [4.3, 19.4] | <0.001 |
| Seropositive (%) | 2258 (78.6) | 2754 (76.8) | 917 (80.1) | 395 (77.0) | 0.087 |
| Previous btsDMARD (%) | <0.001 | ||||
| 0 | 565 (17.2) | 2159 (50.3) | 174 (13.2) | 78 (12.0) | |
| 1 | 973 (29.6) | 1134 (26.4) | 426 (32.4) | 239 (36.8) | |
| 2 | 661 (20.1) | 466 (10.9) | 291 (22.1) | 124 (19.1) | |
| ≥3 | 1092 (33.2) | 530 (12.4) | 424 (32.2) | 208 (32.0) | |
| GC (%) | 1588 (48.4) | 1824 (43.6) | 687 (53.3) | 338 (52.2) | <0.001 |
| csDMARD (%) | <0.001 | ||||
| None | 1521 (48.7) | 1236 (30.9) | 562 (46.9) | 374 (57.8) | |
| Methotrexate | 1040 (33.3) | 1506 (37.7) | 328 (27.4) | 148 (22.9) | |
| Methotrexate and other csDMARD | 189 (6.1) | 552 (13.8) | 134 (11.2) | 50 (7.7) | |
| Other csDMARD | 373 (11.9) | 702 (17.6) | 175 (14.6) | 75 (11.6) | |
| DAS28 | 5.3 [4.2, 6.1] | 5.3 [4.2, 6.1] | 5.3 [4.3, 6.1] | 5.0 [3.8, 5.9] | 0.026 |
| CDAI | 27.4 [18.0, 36.5] | 26.0 [17.0, 35.0] | 24.6 [17.0, 34.2] | 24.2 [16.3, 34.8] | 0.001 |
| CRP | 2.6 [1.0, 6.0] | 3.0 [1.0, 7.9] | 1.0 [0.5, 3.0] | 4.4 [1.9, 10.2] | <0.001 |
| HAQ | 1.2 [0.9, 1.8] | 1.1 [0.6, 1.8] | 1.2 [0.8, 1.9] | 1.2 [0.8, 1.9] | <0.001 |
| Pain | 30.5 [15.0, 52.0] | 35.0 [15.0, 55.0] | 40.0 [20.0, 60.0] | 43.0 [20.0, 65.0] | <0.001 |
All results are median [with interquartile range] or number of patients (indicated with %). BMI, body mass index; CDAI, clinical disease activity index; DAS28, Disease Activity Score in 28 joints; HAQ, health assessment questionnaire; GC, Glucocorticoids.
Trajectories analysis of CDAI . Observed trajectories (left) and adjusted analysis (right) showing short-term evolution of CDAI over time by drug, for the full population (upper panels) and patients taking glucocorticoid (lower panels). ABA: abatacept; CDAI: clinical disease activity index; IL6i: IL-6 inhibitors; JAKi: JAK-inhibitors; TNFi: TNF-inhibitors.
Conclusion: Short-term effectiveness differed significantly, albeit with a relatively small effect, between b/tsDMARDs, with a faster CDAI improvement rate in patients receiving JAKi compared to TNFi. This difference was more pronounced in patient concomitantly treated with GC. Short term GC use may be of interest with all second line therapies when a very rapid response is needed.
REFERENCES: NIL.
Acknowledgements: This study is investigator initiated. The JAK-pot collaboration is supported by unconditional/unrestricted research grants from AbbVie Inc., Eli Lilly and Co., and Alfasigma S.p.A., and was previously supported by Pfizer Inc and Galapagos NV.
Disclosure of Interests: Delphine Sophie Courvoisier: None declared, Matthias Jarlborg: None declared, Denis Mongin: None declared, Romain Aymon: None declared, Roberto F. Caporali: None declared, Denis Choquette: None declared, Catalin Codreanu: None declared, Louis Coupal: None declared, Doreen Huschek: None declared, Kimme Hyrich Abbvie, Pfizer BMS, Florenzo Iannone Abbvie, Alfasigma, Amgen, Astra-Zeneca, Csl-Vifor, GSK, Janssen, Novartis, Lilly, UCB, Abbvie, Amgen, Astra-Zeneca, Janssen, Lilly, UCB, Tore K. Kvien Grünenthal, Janssen, Sandoz, AbbVie, Gilead, Janssen, Novartis, Pfizer, Sandoz, UCB, AbbVie, BMS, Galapagos, Novartis, Pfizer, UCB, Ruth Fritsch-Stork: None declared, Dan Nordström Pfizer, UCB, BMS, Lilly, MSD, Novartis, Pfizer, UCB, BMS, MSD, UCB, Nina Trokovic: None declared, Lucía Otero-Varela: None declared, Karel Pavelka AbbVie, Eli Lilly, Sandoz, UCB, Medac, Pfizer, Sella Aarrestad Provan: None declared, Ana Maria Rodrigues: None declared, Ziga Rotar Abbvie, Amgen, AstraZeneca, Boehringer, Biogen, Eli Lilly, Janssen, Medis, MSD, Novartis, Pfizer, Sandoz Lek, Stada, SOBI, Abbvie, AstraZeneca, Boehringer, Eli Lilly, Janssen, Medis, MSD, Novartis, Pfizer, Sandoz Lek, SOBI, Prodromos Sidiropoulos: None declared, Anja Strangfeld AbbVie, Galapagos, Lilly, Pfizer, Takeda, UCB, Unconditional grant to my institution for the RABBIT register with equal parts from AbbVie, Amgen, BMS, Celltrion, Fresenius Kabi, Galapagos, Hexal, Lilly, MSD, Viatris, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. Jakub Závada Abbvie, Elli-Lilly, Sandoz, Novartis, Egis, UCB, Sanofi, AstraZeneca, Sobi, Abbvie, Novartis, AstraZeneca, Glaxo, Sizheng Steven Zhao Novartis, UCB, AlfaSigma, AbbVie, Novartis, UCB, AlfaSigma, Axel Finckh AbbVie, Astra Zeneca, Eli-Lilly, Pfizer, UCB, Kim Lauper Pfizer.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (