fetching data ... 
Background: Systemic vasculitides are complex and heterogeneous diseases with overlapping features that frequently pose a diagnostic challenge to clinicians. Temporal artery biopsy (TAB) is the procedure with the highest specificity for the diagnosis of GCA. Occasionally, the TAB shows small vessel vasculitis (SVV) surrounding a normal temporal artery as the only pathological finding. Ultimate diagnosis and, consequently, optimal treatment remain uncertain in these patients.
Objectives: To identify differentially expressed genes in TAB with SVV surrounding a spared temporal artery from patients with GCA and other systemic vasculitis including AAV.
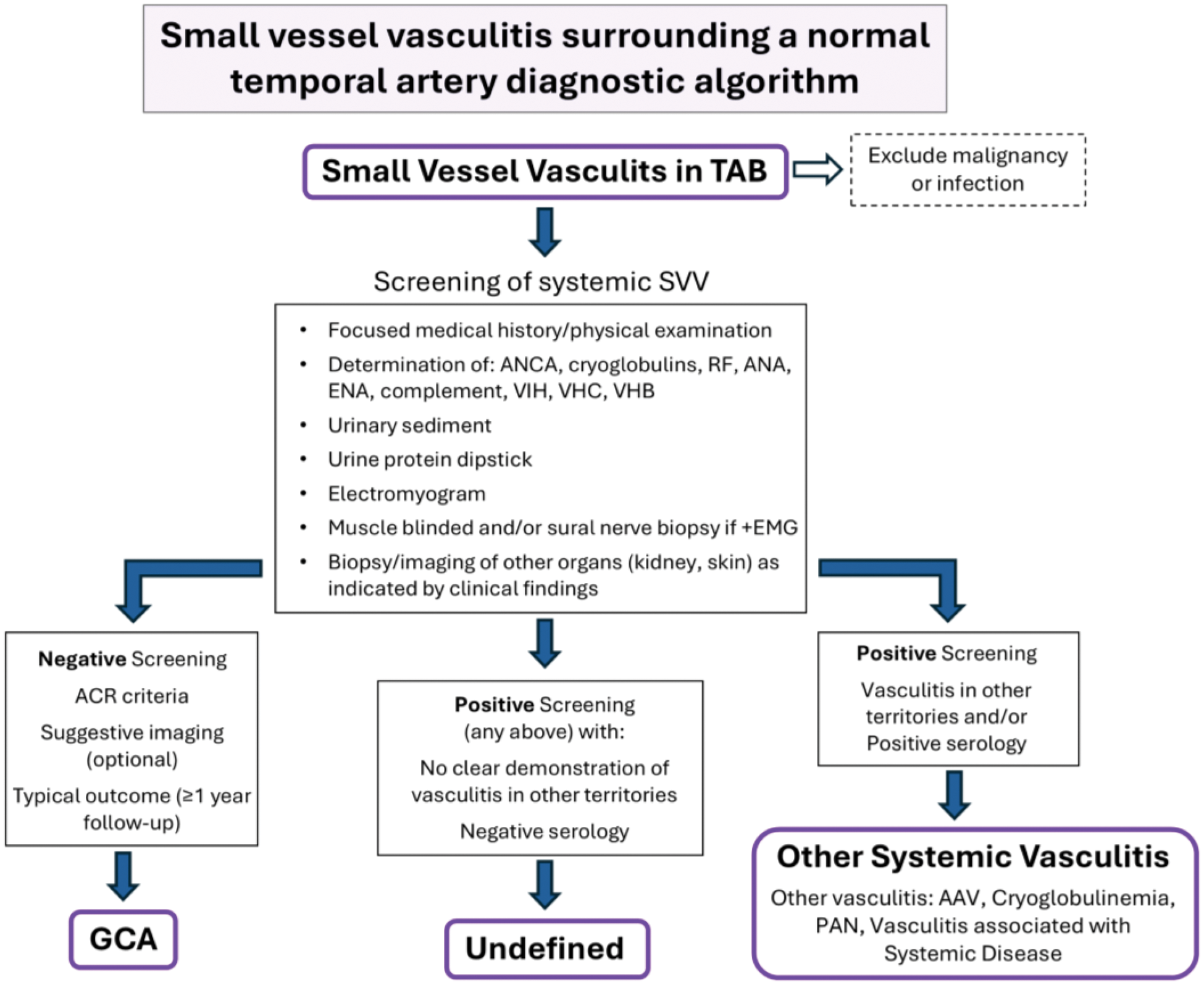
Methods: 51 patients with TAB showing SVV surrounding a normal temporal artery were subjected to a pre-established diagnostic algorithm combining clinical, imaging and serological data (Figure 1). The algorithm led to the following classification: 19 GCA; 20 systemic vasculitis (AAV and other vasculitis); and 12 could not be classified. TAB samples from 16 SVV patients (8 classified as GCA [SVV-GCA] and 8 as systemic vasculitis [SVV-SV]: 4 AAV and 3 other vasculitis) and 16 controls with negative temporal artery biopsies, were used for RNA isolation and microarray hybridization (Human Clariom S, Affymetrix). Data processing and differential expression profiling (p < 0.001) were implemented using Bioconductor. An empirical Bayes moderated t-test was applied for statistical evaluation. To identify patient clusters with similar characteristics, unsupervised hierarchical clustering and principal component analysis (PCA) were implemented.
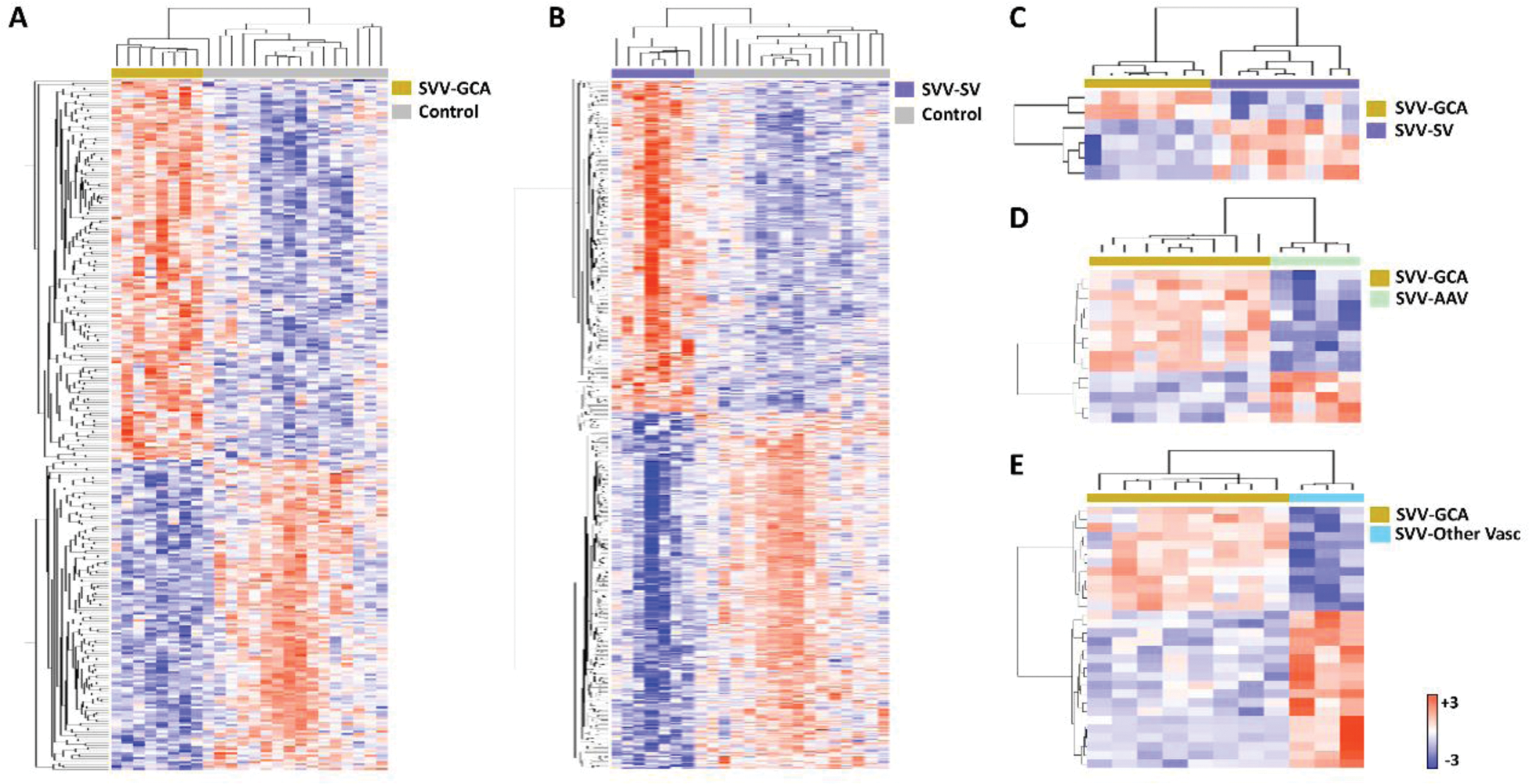
Results: We compared gene expression in normal temporal arteries and in different subgroups of SVV. The expression level of 313 genes was found to be significantly different between normal arteries and SVV-GCA, whereas the expression level of 544 genes was significantly different between normal arteries and SVV-SV. These DEGs were used to perform an unsupervised hierarchical clustering of these groups (Figure 2A and 2B), resulting in their classification into different clusters, each corresponding to their respective phenotype. Moreover, an additional clustering was performed using 6 DEGs, found when comparing SVV-GCA and SVV-SV, distinguishing them into two different clusters (Figure 2C). Sub-analysis between SVV-GCA vs SVV-AAV (Figure 2D), and SVV-GCA vs SVV-other vasculitis (Figure 2E) showed significant differences in expression level of 15 and 30 genes, respectively.
Conclusion: SVV surrounding a spared TA is a relevant but equivocal finding. After a detailed diagnostic work-up most patients can be diagnosed with GCA, AAV or other systemic vasculitis although diagnosis remains uncertain in some cases. Cluster analysis of the gene expression profile differentiates diagnostic subgroups of SVV. Further studies are needed to validate differentially expressed genes. “Supported by PI15/00092, Plan Estatal de Investigación Científica y Técnica de Innovación 2013-2016 y cofinanciado por el ISCIII-Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER)”.
Patients with TAB were subjected to this algorithm.
Unsupervised hierarchical clustering of different subgroups of SVV compared to normal temporal arteries and among them. A) SVV-GCA vs control, B) SVV-SV vs control, C) SVV-GCA vs SVV-SV, D) SVV-GCA vs SVV-AAV, E) SVV-GCA vs SVV-Other Vasculitis.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: Núria Farran: None declared, Roser Alba-Rovira: None declared, Salvador Naranjo-Suárez: None declared, Sergio Prieto-González Roche, Marc Corbera-Bellalta: None declared, Javier Marco-Hernández: None declared, Nina Visocnik: None declared, Maria C. Cid GSK, AstraZeneca, AbbVie and CSL-Vifor, GSK, CSL-Vifor, AstraZeneca, AbbVie, Alexion, Novartis, Boehringer-Ingelheim and Royalty Pharma, Kiniksa Pharmaceuticals, Georgina Espígol-Frigolé GSK and CSL-Vifor, GSK and CSL-Vifor, GSK.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (