fetching data ... 
Background: Immune checkpoint inhibitors (ICIs), a class of cancer immunotherapies, are associated with immune-related adverse events, including musculoskeletal symptoms such as arthritis (ICI-arthritis) and arthralgia (ICI-arthralgia). The latter is very common, affecting up to 50% of patients who receive ICIs. The prevalence and characteristics of ICI-related musculoskeletal adverse events remain poorly defined, with limited imaging data available, especially regarding the subclinical inflammatory burden in ICI-arthralgia. Ultrasound, a sensitive tool for detecting subclinical inflammation, could play a key role in understanding and managing ICI-induced arthritis and arthralgia by enabling earlier diagnosis and intervention.
Objectives: To explore the prevalence and distribution of ultrasound findings of ‘active’ inflammation and structural damage in the joints, tendons, and entheses in patients with ICI-arthralgia, compared to ICI-arthritis patients.
Methods: Cancer patients who developed clinical arthritis (joint pain and swelling on physical examination) or arthralgia (joint pain without clinical arthritis) after receiving ICIs were consecutively recruited across six centres internationally. All participants underwent clinical and ultrasound evaluations. Ultrasound assessments included 18 joints bilaterally (for synovitis and bone erosions), 10 tendons (for tenosynovitis and tendon damage), and 5 entheses (for “active” enthesitis and entheseal bone erosions) at various anatomical sites, using the Outcome Measures in Rheumatology (OMERACT) definitions (1). Statistical analyses, including chi-square and Fisher’s exact tests, compared the prevalence and distribution of ultrasound-detected inflammation between the two groups.
Results: This multi-centre study included 101 patients: 48 with ICI-arthritis and 53 with ICI-arthralgia. The majority of patients had a diagnosis of melanoma (32.7%) or lung cancer (21.8%). Monotherapy (91.1% of patients) with pembrolizumab (46.5%) and nivolumab (30.7%) were the most commonly used treatments. The overall mean age was 63.6 years, with ICI-arthritis patients being older (69.4 years) than ICI-arthralgia patients (64.4 years, p=0.015). C-reactive protein (CRP) levels and early morning stiffness were similar between the two groups. Corticosteroid use was more common in ICI-arthritis patients (59.6%) than in ICI-arthralgia patients (32.7%, p=0.009). There were no significant differences in autoantibody positivity (CCP, ANA, RF) or other immune-related adverse events (44.2% vs. 47.7%, p=0.84). ICI-arthritis patients had monoarthritis (n=18), oligoarthritis (n=15), or polyarthritis (n=15). A high proportion of ICI-arthralgia patients had ultrasound-detected subclinical synovitis (47.2%), tenosynovitis (18.9%), and enthesitis (24.5%) despite the absence of joint swelling (Table 1). Overall, ultrasound synovitis was more frequent in ICI-arthritis than in ICI-arthralgia (93.8% vs. 47.2%, p<0.001), particularly in the wrists (56.3% vs. 20.8%, p<0.001) and knees (54.2% vs. 13.2%, p<0.001), which were the most frequently affected joints. Tenosynovitis was also more common in ICI-arthritis (52.1% vs. 18.9%, p<0.001), most frequently seen at the extensor carpi ulnaris (22.9% vs. 9.2%, p=0.1). However, there was no significant difference in the prevalence of “active” enthesitis (31.3% vs. 24.5%, p=0.51), which was most common at the lateral epicondyles in both groups. Bone erosions were more prevalent in ICI-arthritis than in ICI-arthralgia (25% vs. 7.5%, p=0.027), most commonly seen at the wrists (ulnar styloid) in both groups (16.7% vs. 5.7%, p=0.11). A pictorial example of joint synovitis, tenosynovitis and enthesitis in patients with ICI-arthritis/arthralgia is shown in Figure 1.
Conclusion: These multi-national cohort data represent the largest and most comprehensive ultrasound study of patients with ICI-arthritis and ICI-arthralgia. ICI-arthritis demonstrated a large inflammatory and structural burden, especially at the wrists and knees. Sonographic patterns were heterogeneous, with varying involvement of joints, tendons, and entheses. There was a high frequency of ultrasound-detected subclinical inflammation in ICI-arthralgia, with synovitis identified in almost half of all patients. These findings suggest that subclinical inflammation may often be responsible for the common presentation of arthralgia after ICI exposure. Rheumatological ultrasound assessment should be routinely considered in these patients to facilitate early, accurate diagnosis and more tailored interventions.
REFERENCES: [1] Bruyn GA, et al. OMERACT Definitions for Ultrasonographic Pathologies and Elementary Lesions of Rheumatic Disorders 15 Years On. J Rheumatol. 2019.
Table 1 . Prevalence and distribution of the ultrasound findings in patients with ICI-arthritis and arthralgia.
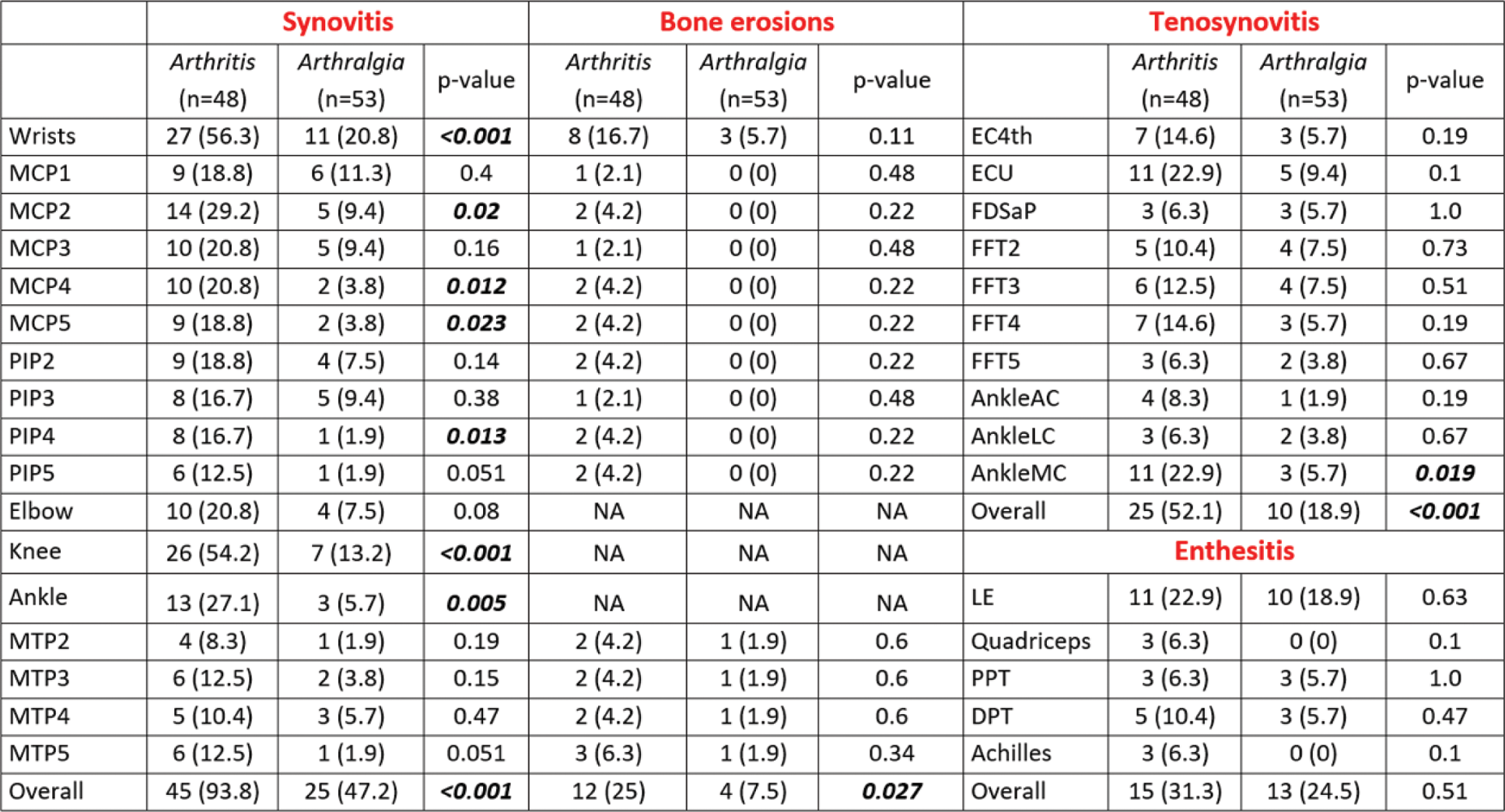
Legend . Results are reported as numbers with percentage. Acronyms: AC: Anterior Compartment; DPT: Distal Patellar Tendon; ECU: Extensor Carpi Ulnaris; FDSaP: Flexor Digitorum Superficialis and Profundus; FFT: Finger Flexor Tendons; LC: Lateral compartment; LE: Lateral Epicondyle; MC: Medial Compartment; MCP: Metacarpophalangeal Joint; MTP: Metatarsophalangeal Joint: NA: Not Applicable; PIP: Proximal Interphalangeal Joint; PPT: Proximal Patellar Tendon.
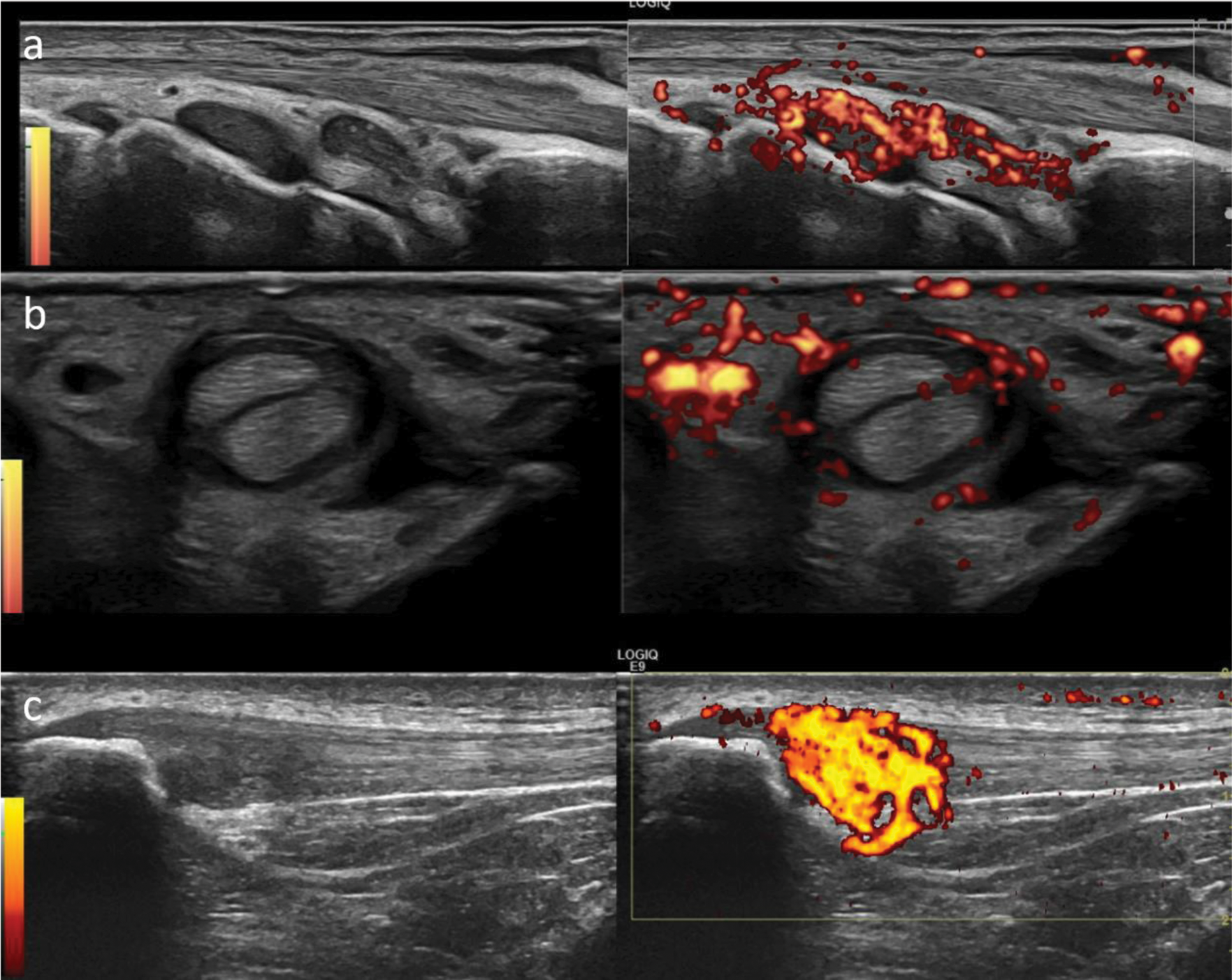
Pictorial examples of joint synovitis, tenosynovitis and enthesitis in patients with ICI-arthritis
Legend . Images show wrist synovitis (a), 3rd finger flexor tendon tenosynovitis (b) and proximal patellar tendon enthesitis (c).
Acknowledgements: NIL.
Disclosure of Interests: Andrea Di Matteo Janssen, Kate Harnden: None declared, Sana Sharrack: None declared, Kerem Abacar: None declared, Luca Di Geso: None declared, Rudolf Horvath: None declared, Jana Hurnakova: None declared, Tadashi Okano: None declared, Didem Sahin Eroglu: None declared, Paraskevi V. Voulgari: None declared, Juan Jose de Agustin: None declared, Emilio Filippucci: None declared, Paul Emery Abbvie, Activa, Astra-Zeneca, BMS, Boehringer Ingelheim, Galapagos, Gilead, Immunovant, Janssen, Lilly, Novartis, Abbvie, Activa, Astra-Zeneca, BMS, Boehringer Ingelheim, Galapagos, Gilead, Immunovant, Janssen, Lilly, Novartis, Kulveer Mankia Abbvie, ALLin Bio, Astra Zeneca, UCB, Lilly, Galapagos, Serac Healthcare, Zura Bio, Deepcure, Gilead, Lilly, Serac Healthcare, Astra Zeneca, Deepcure.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (