fetching data ... 
Background: The well-known increased cardiometabolic risk in psoriatic arthritis (PsA) and the beneficial effect of physical fitness on this risk in both the general population and PsA, highlight the need for a feasible and valid measure of physical fitness in clinical practice. Peak oxygen uptake (VO 2 peak), the gold standard measure of cardiorespiratory fitness (CRF), is assessed during a maximal cardiopulmonary exercise test (CPET), which requires maximal physical effort, safety measures, and specialized equipment. Therefore, submaximal clinical field tests were developed and have shown to be reliable and valid to evaluate different aspects of physical fitness in musculoskeletal conditions [1]. However, clinical field tests assessing submaximal CRF and muscular fitness, e.g. the six minute walk test (6MWT) and handgrip strength test (HGS), have not been studied systematically in PsA.
Objectives: This study aimed to determine the level of submaximal CRF and muscular fitness in patients with PsA compared to the general population and to evaluate the potential of clinical field tests, namely 6MWT and HGS, to be a surrogate for CPET to assess CRF in patients with PsA.
Methods: In this cross-sectional study, submaximal CRF was measured as meters walked during a 6MWT (6MWD; maximum value of two 6MWTs) and muscular fitness as HGS by JAMAR hand dynamometer in kg (maximum value of three attempts at both sides). CRF was measured as peak oxygen uptake (VO 2 peak) during an incremental maximal cardiopulmonary exercise test on a cycle ergometer. 6MWD, HGS, and VO 2 peak were compared to the mean values of the reference population of Marques et al. 2020, the NAKO cohort 2023, and to a Dutch Flemish physically active population (Lowlands Fitness registry 2021) respectively [2, 3, 4]. HGS below percentile five of NAKO cohort 2023 and 6MWD<380m were applied to identify patients with impaired HGS and 6MWD [5]. The one-sided Wilcoxon rank-sum test was used to examine if 6MWD, HGS, or VO 2 peak of patients were significantly decreased compared to the reference population. Spearman’s rank correlation coefficients (r S ) and multivariable linear regression models adjusted for age, sex, and having disease activity in lower limbs were analysed to evaluate the relationship between 6MWD, HGS, and VO 2 peak (log-transformed). Statistical significance was defined as p<.05.
Results: Eighty patients with PsA were included. Demographic characteristics and CRF level are presented in Table 1. 6MWD and HGS of PsA-patients were not significantly lower compared to the general population (Table 1, p>.05). Six and four patients had an impaired HGS and 6MWD respectively (Table 1). VO 2 peak of the patients with PsA was importantly decreased compared to an active reference population (median 73.86% (Q1- Q3 60.99%–87.05%), p<.05). 6MWD was significantly and largely associated with VO 2 peak expressed in ml/min/kg (r S = 0.64 (95%CI 0.49; 0.75), p=.00). The regression model including 6MWD, age, sex, and active disease in lower limbs explained 62% of the variance in VO 2 peak expressed in ml/min/kg (Table 2). HGS was also significantly associated with VO 2 peak (r S = 0.28 (95%CI 0.06; 0.47), p=.02). The regression model including HGS, age, sex, and active disease in lower limbs explained 35% of the variance in VO 2 peak expressed in ml/min/kg (Table 2). Adding HGS to the regression model of 6MWD could not significantly increase the explained variance in VO 2 peak.
Conclusion: Overall, 6MWD and HGS of patients with PsA were similar to the reference population. In this PsA patient population with decreased CRF, both 6MWD and HGS were significantly associated with VO 2 peak with the strongest association observed for 6MWD, suggesting that the 6MWT is a strong candidate for validly evaluating CRF in clinical practice. The use of clinical field tests may facilitate the implementation of physical fitness testing in disease and cardiometabolic risk management of patients with PsA.
Table 1. Demographic characteristics and physical fitness level of included patients with PsA
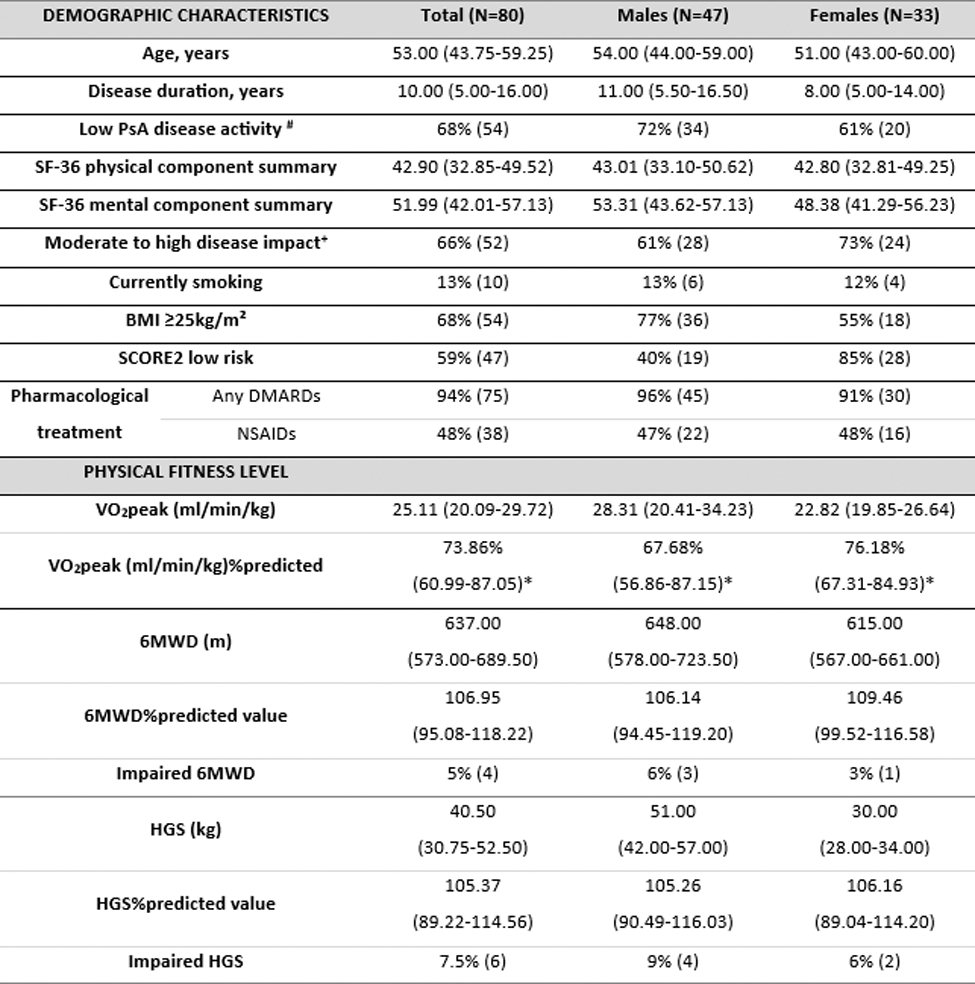
Results presented as median (Q1-Q3) or percentage (N). # PASDAS≤3.2; + PsAID12 >1.95 SCORE2: Systematic COronary Risk Estimation 2. *One-sided Wilcoxon rank-sum test for physical fitness variables: p<.05.
Table 2. Multivariable linear regression models: relation between (1) log(VO 2 peak) and 6MWD and (2) log(VO 2 peak) and HGS
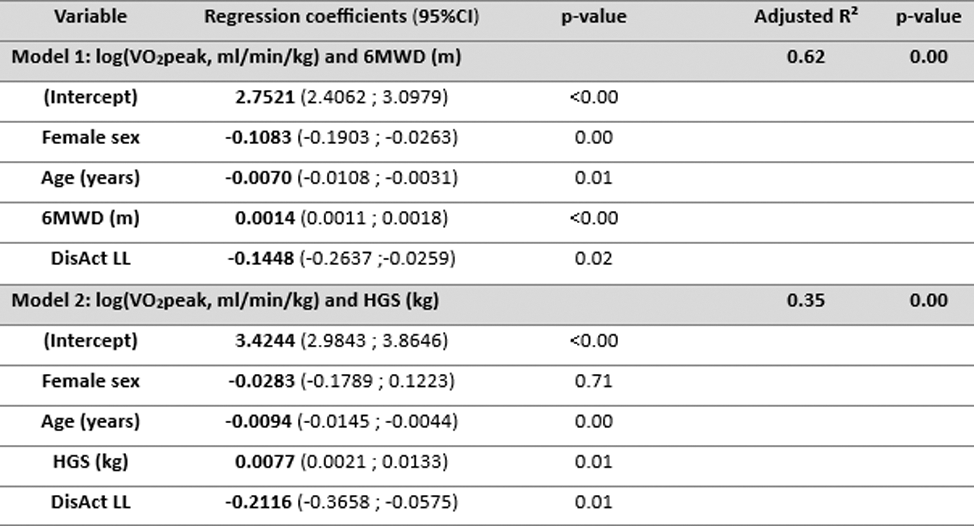
DisAct LL: active rheumatic disease in lower limbs as dichotomous outcome (yes = 1 )
REFERENCES: [ 1] Tveter AT, Dagfinrud H, Moseng T, Holm I. Measuring health-related physical fitness in physiotherapy practice: reliability, validity, and feasibility of clinical field tests and a patient-reported measure. J Orthop Sports Phys Ther 2014;44:206-16.
[2] Marques A, Rebelo P, Paixão C, et al. Enhancing the assessment of cardiorespiratory fitness using field tests. Physiotherapy 2020;109:54-64.
[3] Huemer MT, Kluttig A, Fischer B, et al. Grip strength values and cut-off points based on over 200,000 adults of the German National Cohort - a comparison to the EWGSOP2 cut-off points. Age Ageing 2023;52.
[4] van der Steeg GE, Takken T. Reference values for maximum oxygen uptake relative to body mass in Dutch/Flemish subjects aged 6-65 years: the LowLands Fitness Registry. Eur J Appl Physiol 2021;121:1189-96.
[5] Grundtvig M, Eriksen-Volnes T, Ørn S, Slind EK, Gullestad L. 6 min walk test is a strong independent predictor of death in outpatients with heart failure. ESC Heart Fail 2020;7:2904-11.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (