fetching data ... 
Background: Due to the presence of estrogen and progestin, females are more likely to develop rheumatologic and autoimmune disease compared to males. Estrogen targets type 1 interferons, CD4+ T helper cell differentiation, and B cells. Estrogen has a particularly strong link to Systemic Lupus Erythematosus (SLE) and Rheumatoid arthritis (RA), resulting in a female predominance of both diseases. Presently there is no data exploring the risk of developing autoimmune disease in the transgender population after starting hormone replacement therapy. This study explores the incidence of developing rheumatologic and autoimmune disease in the transgender women and transgender men population on hormone replacement therapy (HRT)- either estrogens or progestin in women or testosterone in men.
Objectives: We designed an observational, retrospective cohort study that aimed to evaluate the incidence of autoimmune and rheumatic disease in both transgender men and women on hormone replacement therapy compared to transgender men and women not on hormone replacement therapy using the TriNetX database, which included electronic health records from >142 global collaborative healthcare organizations.
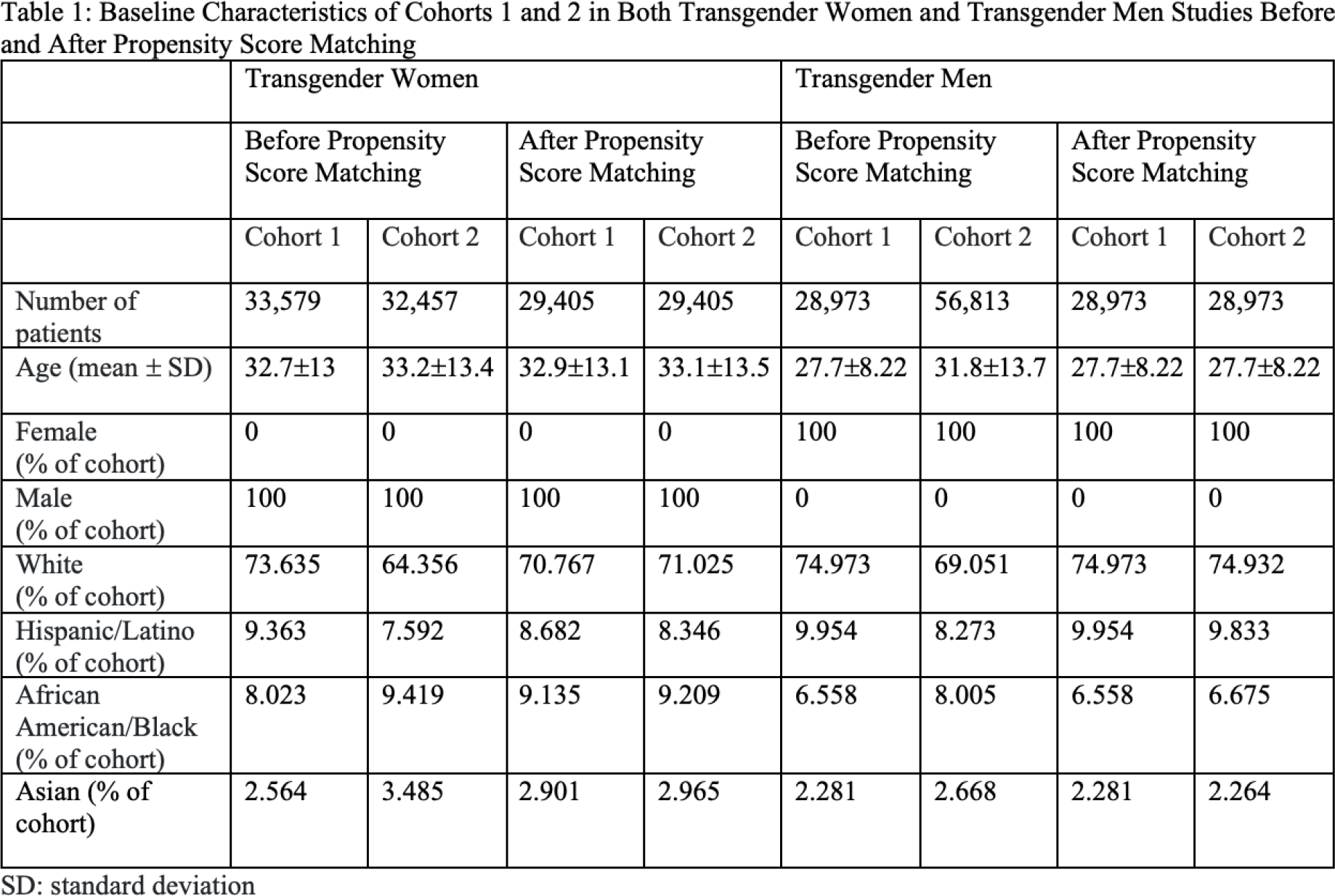
Methods: This study included two populations 18 years and older that were studied separately and were filtered by sex as noted in electronic health records (could be either sex assigned at birth or after legal sex change). The first population studied was transgender women (filtered by sex: men, with a diagnosis of gender dysphoria). Two cohorts were created using the International Classification of Diseases, Tenth Revision (ICD-10) codes: Cohort 1 consisted of transgender females on hormone replacement therapy with estrogens, progestins, or spironolactone and Cohort 2 consisted of transgender women not on hormone replacement therapy. The index event in both cohorts was starting hormone replacement therapy. Propensity score matching was used for the age at index event and race/ethnicity. The second population studied was transgender men (filtered by sex: women, with a diagnosis of gender dysphoria). Two cohorts were created using the International Classification of Diseases, Tenth Revision (ICD-10) codes: Cohort 1 consisted of transgender men on hormone replacement therapy with testosterone and Cohort 2 consisted of transgender men not on testosterone. The index event in both cohorts was starting testosterone. Propensity score matching was used for the age at index event and race/ethnicity. All 4 cohorts were followed over the course of 5 years from January 2021 to January 2026. The primary outcome was the incidence of SLE, Systemic Sclerosis (SSc), Hashimoto’s thyroiditis, RA, Sjogren’s disease, osteoporosis, psoriatic arthritis (PsA), inflammatory bowel disease (IBD), ankylosing spondylitis, and inflammatory myositis.
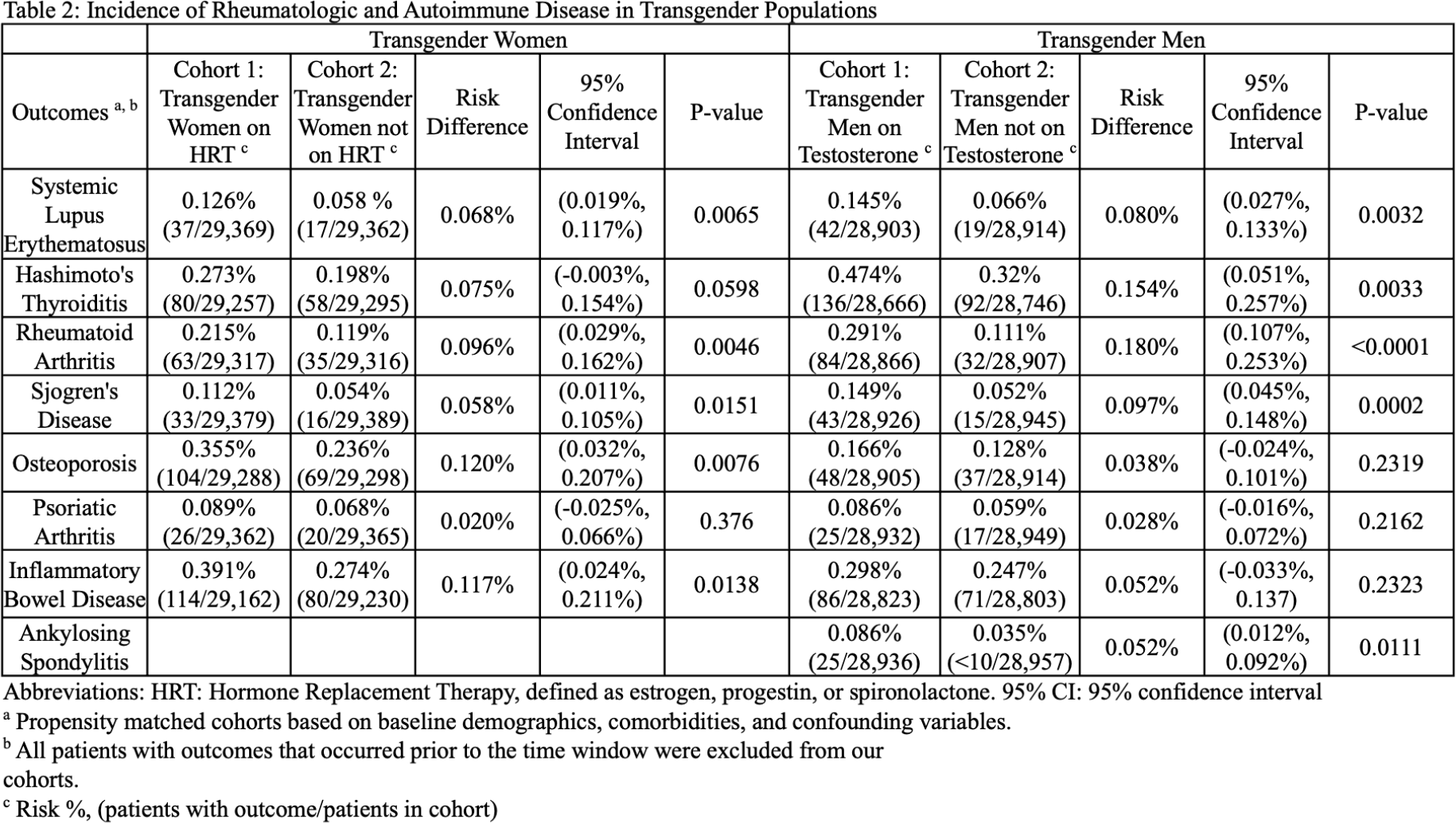
Results: After propensity score matching in the transgender women study, 29,405 patients in each cohort were available for comparative analysis. After propensity score matching in the transgender men study, 28,973 patients in each cohort were available for comparative analysis. See Table 1 for baseline characteristics before and after propensity score matching. Findings from the first study suggest that transgender women on HRT with either estrogens, progestins, or spironolactone have a statistically significant increase in risk of developing SLE, RA, Sjogren’s disease, osteoporosis, and IBD: SLE (Risk difference 0.068%, 95% CI [0.019%, 0.117%], p-value 0.0065), RA (Risk difference 0.096%, 95% CI [0.029%, 0.162%], p-value 0.0046), osteoporosis (Risk difference 0.120%, 95% CI [0.032%, 0.207%], p-value 0.0076). There was no statistically significant risk of developing Hashimoto’s thyroiditis or PsA in the transgender women population on hormone replacement therapy. There was not a large enough sample size to determine if there is a significant risk of developing SSc, ankylosing spondylitis, or inflammatory myositis. Findings from the second study suggest that transgender men on testosterone have a statistically significant increase in risk of developing SLE, Hashimoto’s thyroiditis, RA, Sjogren’s disease, and ankylosing spondylitis: SLE (Risk difference 0.080%, 95% CI [0.027%, 0.133%], p-value 0.0032), RA (Risk difference 0.180%, 95% CI [0.107%, 0.148%], p-value 0.0002), Sjogren’s disease (Risk difference 0.097%, 95% CI [0.045%, 0.148%], p-value 0.0002). There was no statistically significant risk of developing osteoporosis, PsA, or IBD in the transgender men population on testosterone. Sample size was not large enough to determine if there is a significant risk of developing SSc or inflammatory myositis.
Conclusions: Despite being born genetically male, transgender women on HRT have an increased risk of developing SLE, RA, Sjogren’s and osteoporosis, diseases more commonly seen in females. Whereas transgender men on testosterone have an increased risk of developing SLE, Hashimoto’s thyroiditis, RA, Sjogren’s disease, and ankylosing spondylitis. Testosterone supplementation does not seem to be enough to overcome this population’s genetics and hormones from birth, particularly estrogen. Limitations of this study include ICD-10 coding discrepancies for the transgender population. If transgender patients are not on hormone replacement therapy, physicians may not document their orientation as an ICD-10 code, leading to a falsely smaller sample size. Also patient’s sex in the electronic health record may not represent their sex at birth. If patients pursue legal sex change, documentation is skewed. Further research should be conducted with a larger population size, with for a longer duration than 5 years, with more accurate cohorts to confirm these associations.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.