fetching data ... 
Background: Juvenile Idiopathic Arthritis (JIA) is the most common form of chronic arthritis in childhood. The adaptive branch of the immune system plays a crucial role in the development of JIA. An hyperactivation of B cells characterizes patients with oligoarticular- and polyarticular-JIA (Barnes MG, A&R 2010) and we have showed that switched memory B cells are expanded in this group of patients (Marasco E, A&R 2018). Preliminary data from our group showed that B cells of JIA patients showed changes in the immunoglobulin repertoire with an altered peripheral selection process and lower frequency of somatic hypermutation, suggesting an extrafollicular activation of autoreactive B cells.
Objectives: Building on our previous work, we aimed to investigate the phenotype of B cells in patients with JIA.
Methods: Paired mononuclear cell samples isolated from peripheral blood (PBMC) and synovial fluid (SF) of JIA patients were retrospectively retrieved from our biobank (n = 15 patients with paired samples). B- and T-cell immunophenotypes were characterized by conventional multiparametric flow cytometry. Intracellular T-bet expression in CD19 + cells (n=14 patients with paired samples) was assessed according to a previously published protocol (Moneta G, EJI 2023). Pediatric controls were recruited at our department among children who referred for growing pains or recurrent fevers, for whom a rheumatological disease was excluded. B cell phenotype data were confirmed in an independent cohort of JIA patients (n=49) for whom a blood sample was available in our biobank at baseline and patients were followed up for a minimum of three years after diagnosis. Levels of BAFF and CXCL13 were evaluated by ELISA (R&D Systems). For TLR9 activation PBMCs were loaded with CFSE and stimulated in vitro with CpG as previously described (Marasco E, EJI 2017) for seven days, plasmablasts were identified as CD19+CD27++CD38++.
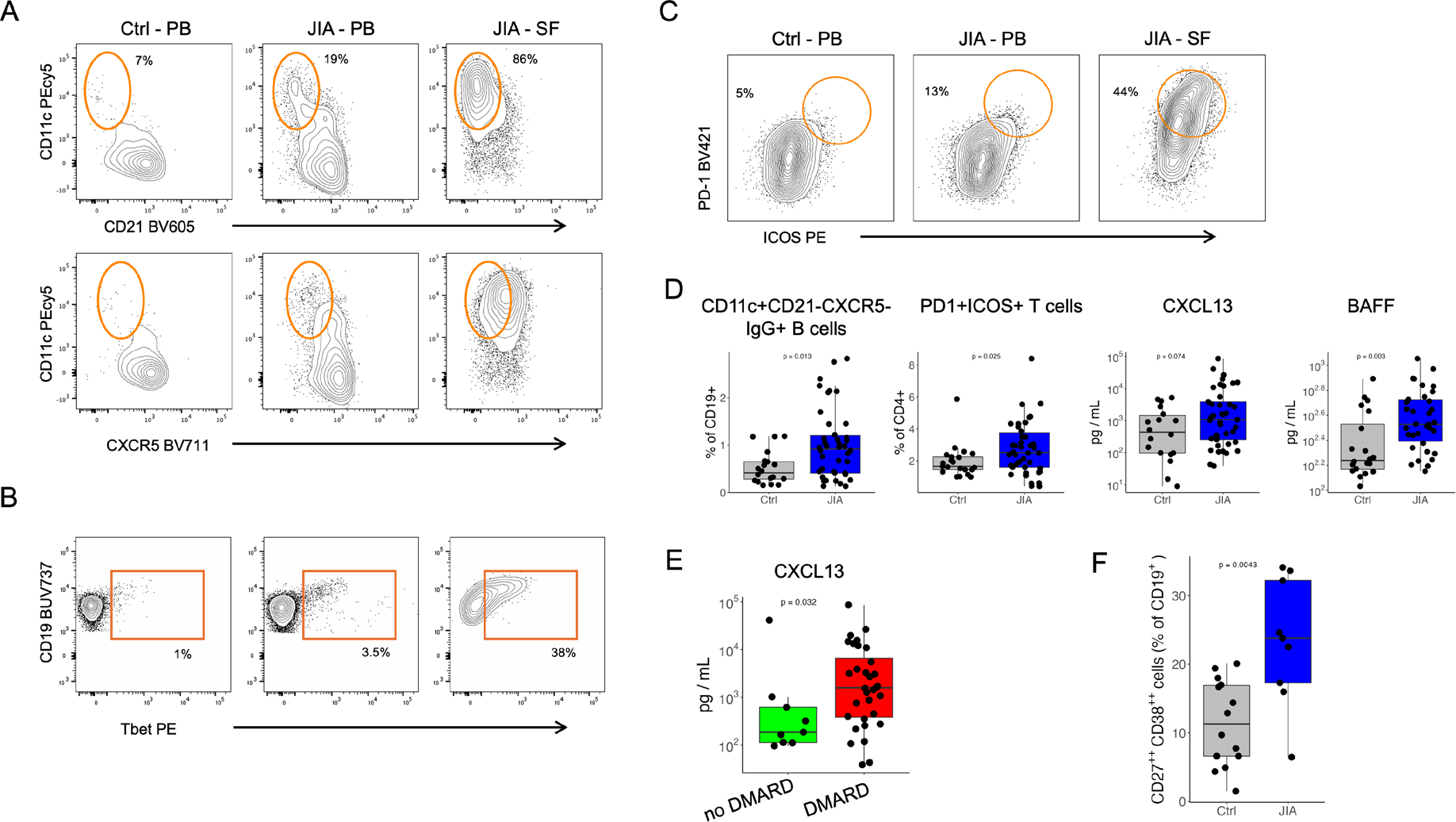
Results: We enrolled 15 patients with a diagnosis of JIA according to the ILAR criteria. Ten (67%) patients had a diagnosis of oligoarticular-JIA, five (33%) RF negative poly-JIA; 11 patients (74%) were female. Five (34%) patients were on methotrexate, nine (60%) patients were on methotrexate + TNF inhibitor, one (6%) patient was on TNF inhibitor alone. The ratio of IgG to IgA memory B cells was higher in JIA patients than controls, indicating and expansion of IgG+ memory B cells in JIA. IgG+ memory B cells were the most abundant B cell subset in SF. The phenotype of IgG+ memory B cells showed an enrichment for CD21-CXCR5-CD11c+ especially in SF, suggesting an extrafollicular origin (Figure 1A). We performed intracellular staining for Tbet, a transcription factor that plays a role in extrafollicular responses: Tbet+ B cells were expanded in SF compared to PB of patients with JIA and controls (Figure 1B). We found activated ICOS+ PD1+ peripheral helper T cells (Tph) enriched in SF compared to PB of patients and controls (Figure 1C).
Our validation cohort consisted of 49 children with JIA: 42 (85%) had oligo-JIA and seven (15%) had RF- poly-JIA; 33 (68%) were female; median age at diagnosis was 5.1 years (IQR 2.8 -7.2). We evaluated the frequency of CD21-CXCR5-CD11c+ B cells and Tph in this validation cohort and also assessed the plasma levels of BAFF and CXCL13. We confirm the expansion of CD21-CXCR5-CD11c+IgG+ B cells in patients compared to controls (Figure 1D). Patients at diagnosis also showed higher levels of BAFF and CXCL13 and an expansion of Tph cells (Figure 1D). We then separated patients in two groups based on the follow up data: patients who were treated only with joint injection (no DMARDs) and patients who had to start methotrexate or a TNF inhibitor (DMARD) for active disease after joint injections. Patients in the DMARD group showed higher levels of CXCL13, whereas levels of CD21-CXCR5-CD11c+IgG+ B cells, Tph cells and BAFF were comparable between the two groups (Figure 1E).
TLR9 plays a central role in activating B cells in the extrafollicular areas. We stimulated cells of JIA patients (n=9) and controls (n=14) with CpG: after 7 days the fraction of plasmablasts was higher in patients than controls (Figure 1F).
Conclusions: Our findings indicate that JIA is characterized by enhanced extrafollicular B cell activation, accompanied by an expansion of Tph cells that can provide B cell help outside germinal centers. BAFF and TLR9 signaling likely contribute to this extrafollicular activation program. In parallel, we detected increased CXCL13 levels, consistent with augmented follicular B cell responses. CXCL13 elevation was most evident in patients who went on to require systemic therapy. Together, these data support a model in which extrafollicular B cell activation is a core feature of JIA, whereas heightened follicular responses (occurring in lymph nodes or synovial tertiary lymphoid structures) may mark a subset of patients with more severe disease who require systemic treatment.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Emiliano Marasco: None declared, Andrea Ariolli: None declared, Nina De Franco: None declared, Angela Aquilani: None declared, Giusyda Tarantino: None declared, Maria Isabella Petrone: None declared, Rebecca Nicolai: None declared, Ivan Caiello: None declared, Silvia Magni-Manzoni: None declared, Fabrizio De Benedetti Member of the Data Safety Monitoring Board for Regeneron; consultant for Sobi, Novartis, and Apollo., Unrestricted research grants from Sobi, Sanofi, Regeneron, Roche, Elixiron, and Novartis.