fetching data ... 
Background: Advances in understanding rheumatoid arthritis (RA) pathogenesis have led to the development of highly effective therapies, particularly when introduced early in the disease course. Prompt diagnosis and tight disease control can prevent or limit structural joint damage. Nevertheless, up to 40% of patients show an inadequate therapeutic response, and sustained clinical remission remains uncommon, reflecting disease heterogeneity. Synovial tissue studies have revealed diverse histopathological and molecular patterns associated with different levels of disease activity and treatment response. However, the relationship between synovial features at disease onset and long-term outcomes remains poorly defined.
Objectives: To identify clinical, histological, and molecular determinants of 5-year disease remission in patients with early Rheumatoid Arthritis undergoing synovial biopsy at disease onset.
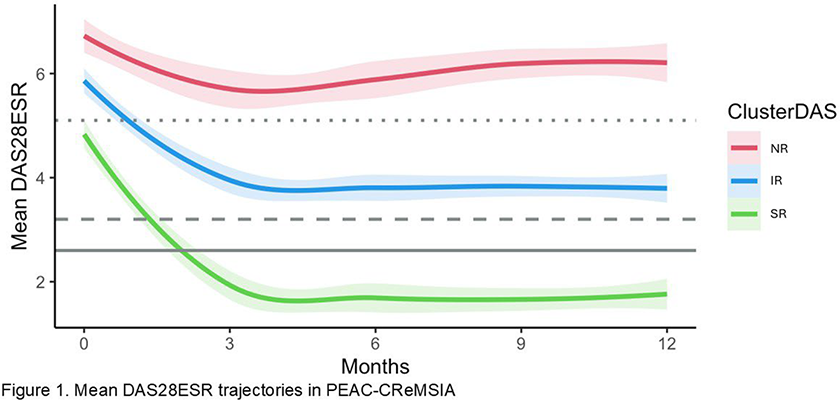
Methods: Patients with treatment-naïve early (<12m) RA were recruited in The Pathobiology of Early Arthritis Cohort (PEAC) and underwent an ultrasound-guided synovial biopsy of a clinically active joint (Synovial thickening≥2). Patients were treated according to a treat-to-target strategy with a combination of DMARDs aiming for low disease activity (DAS28≤3.2). Immunohistochemistry was performed and samples were classified into lympho-myeloid, diffuse-myeloid, or pauci-immune pathotypes, as previously described. Matched samples underwent bulk RNA sequencing. 106 participants who consented to long-term follow-up via the Clinical Records Management System for Inflammatory Arthritis (CReMSIA) registry had clinical outcomes collected over 60 months. Baseline clinical, histological, and transcriptional features were compared, including differential gene expression analyses, against 60-month disease activity outcomes: remission/low disease activity (Rem/LDA; DAS28 ≤3.2) versus moderate/high disease activity (MDA/HDA; DAS28 >3.2). Longitudinal disease trajectories were examined using DAS28 values at baseline and at 3, 6, 9, and 12 months. Data were available for 76 patients. Clustering was performed with k-means for longitudinal data (KML) approach, using Euclidean distance and k-means++ initialisation. Missing data were imputed by a local linear interpolation method, and the optimal number of clusters was fixed at three based on clinical interpretability.
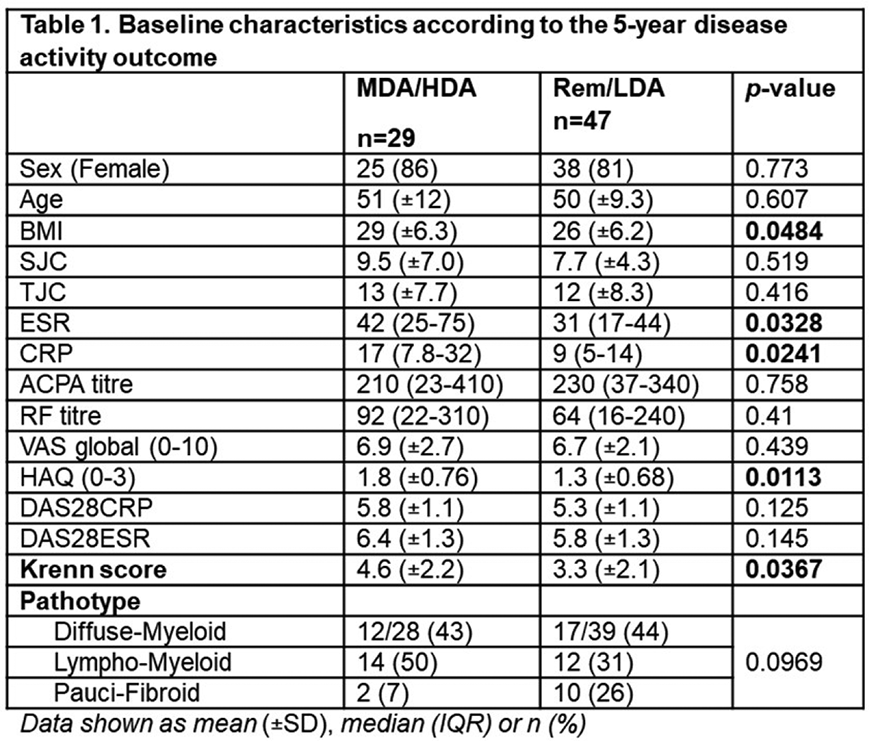
Results: At baseline, median age was 50 years (IQR 40-56), and 77% were female. Median disease activity was high, with a median DAS28 of 5.9 (IQR 4.9-6.9), tender joint count (TJC) of 11 (IQR 5-17), and swollen joint count (SJC) of 6.5 (IQR 3-10). Histological classification (n=93) showed typical early RA pathotype distribution: lympho-myeloid 40%, diffuse-myeloid 38%, pauci-immune 22%. At 60 months, median DAS28 was 2.8 (IQR 2.1-4), with 42% of patients in Rem and 17% in LDA. Regarding treatment, 42% of patients were receiving one csDMARD, 36% two csDMARDs, and 29% a bDMARD. Overall, 82% had no prior exposure to bDMARDs before the 60-month assessment. Patients achieving Rem/LDA at 60 months (n=29) had significantly lower baseline BMI (26±6.2 vs 29±6.3, p=0.0484), ESR (median 31, IQR 17–14 vs 42, IQR 25–75, p=0.0328), CRP (median 9, IQR 5–14 vs 17, IQR 7.8–32, p=0.0241), HAQ score (1.3±0.68 vs 1.8±0.76, p=0.0113), and Krenn score (3.3±2.1 vs 4.6±2.2, p=0.0367) compared with the MDA/HDA group (n=47) (Table 1). Importantly, treatment exposure over the 60-month follow-up did not differ between the two groups. Baseline synovial transcriptomics in Rem/LDA patients at 5-years showed enrichment of cytoskeletal and connective tissue organisation, oxygen and ion transport, and negative regulation of inflammatory pathways (including NF-κB), alongside downregulation of metabolic and biosynthetic pathways, endoplasmic reticulum and oxidative stress responses, apoptotic and protein homeostasis processes, developmental and signalling pathways (including Notch signalling), and regulation of glucose and carbohydrate metabolism pathways. Trajectory-based clustering over the first 12 months identified three disease patterns: super-responders (SR), with rapid and sustained remission; inadequate-responders (IR), with persistently moderate disease activity; and non-responders (NR), with high disease activity. The proportion of females was lowest in the SR group (57% vs 71% vs 88%, p=0.00236). At baseline, SR patients had lower DAS28, TJC, SJC, ESR, CRP, and patient-reported outcomes than IR and NR (all p≤0.01). These differences persisted at 60 months, with significantly lower DAS28 (p=0.0125), ESR (p=0.00364), TJC (p=0.0225), and VAS global score (p=0.0305) in SR patients. SR patients also required biologic therapy less frequently (p=0.0378), and were more often bDMARD-free than IR and NR (86%, 67%, and 57%, respectively).
Conclusions: In early rheumatoid arthritis, baseline clinical burden and synovial molecular features are key determinants of long-term disease control. Patients achieving sustained remission or low disease activity at 60 months had lower inflammatory markers and milder synovial inflammation at diagnosis. Downregulation of stress and biosynthetic pathways, together with upregulation of tissue differentiation and anti-inflammatory pathways, indicates a resolution-prone synovial pathotype detectable at disease onset. Trajectory analyses identified a subgroup of super-responders characterised by rapid disease suppression, sustained remission reflecting a favourable disease course rather than a treatment-specific response. Together, these findings underscore the prognostic value of early clinical, histological, and molecular profiling, suggesting that intrinsic disease biology, rather than treatment intensity alone, drives long-term outcomes in RA.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.