fetching data ... 
Background: cardiovascular risk excess in rheumatoid arthritis (RA) cannot be explained by traditional risk factors alone. Autoimmunity and immune dysregulation are though to play a role. However, the contribution of adaptive immunity is not completely understood. The production of antibodies against novel (auto)-antigens generated in the context of atherosclerosis has been proposed. Recent experimental data have identified ALDH4A1 as a mitochondrial self-antigen implicated in mouse models of atherosclerosis, yet its clinical significance in human autoimmunity remains unexplored.
Objectives: to characterize ALDH4A1 and anti-ALDH4A1 antibody levels in early RA, to evaluate their associations with atherosclerosis burden and their potential role as biomarker, and to assess their associations with lipid and lipoprotein traits in RA.
Methods: 82 early, untreated RA (2010 EULAR/ACR classification criteria; 69% RF, 66% ACPA; DAS28 5.28±1.13), 14 individuals with clinical-suspect arthralgia (CSA) (EULAR definition; 54% RF, 45% ACPA) and 70 healthy controls (HC) were recruited. A validation cohort consisting of 90 established RA patients (55% RF, 63% ACPA; DAS28 3.58±1.37; median disease duration: 5.66 (0.50-22.83) years; CV events: n=16) and 37 HC was included. A group of 13 bDMARD-naïve RA patients were prospectively followed for 3 months upon TNF blockade initiation. ALDH4A1 and anti-ALDH4A1 antibodies (IgM, IgG, IgA, and IgG subclasses) were measured by commercial and in-house immunoassays. Atherosclerosis occurrence was measured by Doppler-ultrasound. Serum proteins were evaluated through high-throughput targeted proteomics. Lipoprotein profiles (particle class, content, number and size) were assessed by H-NMR. Lipidomic profiles were analyzed by untargeted mass spectrometry (LC-MS/MS). Total cell-free DNA (cfDNA) and nuclear (n) or mitochondrial (mt) fractions were assessed in plasma by fluorometry and qPCR.
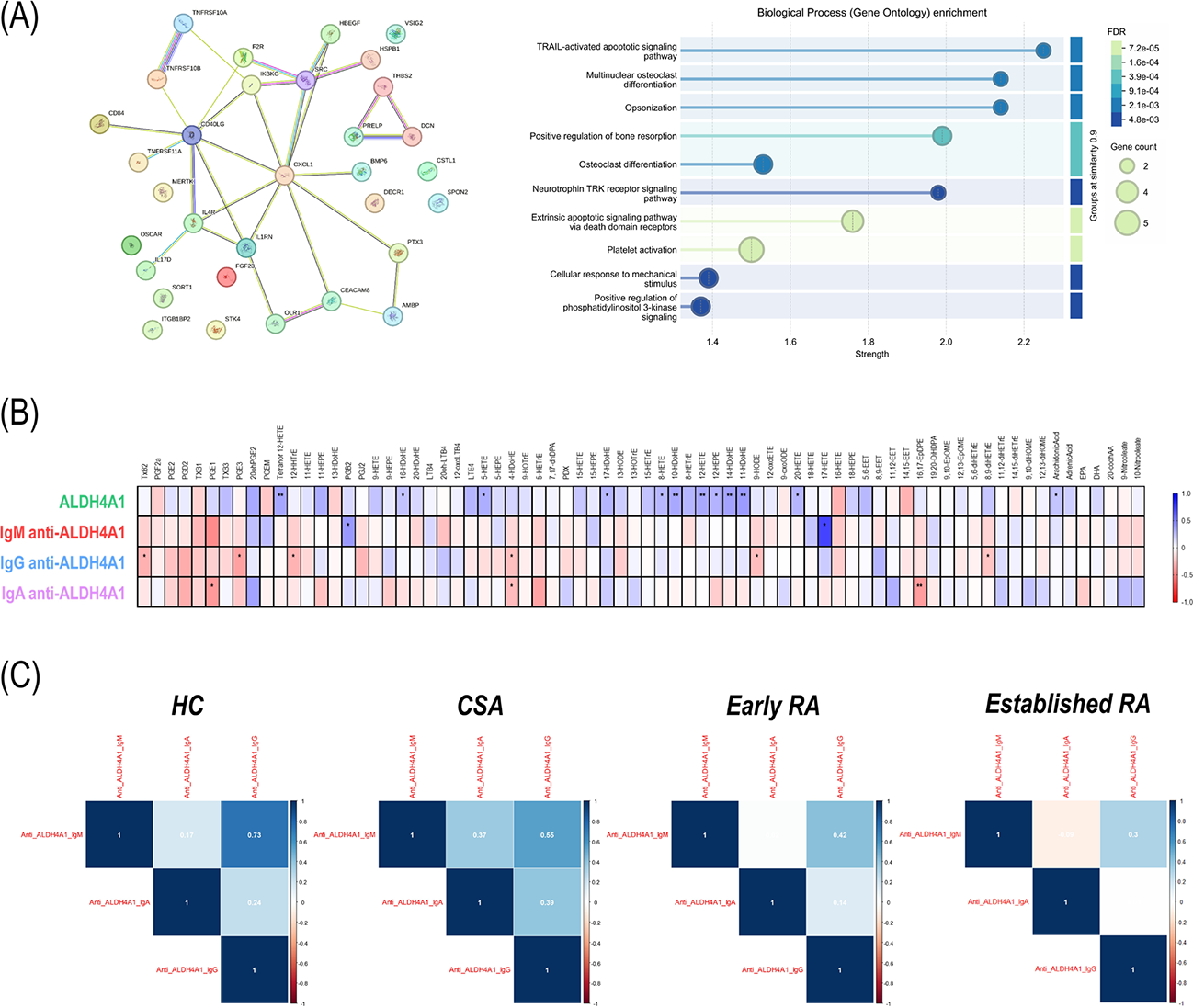
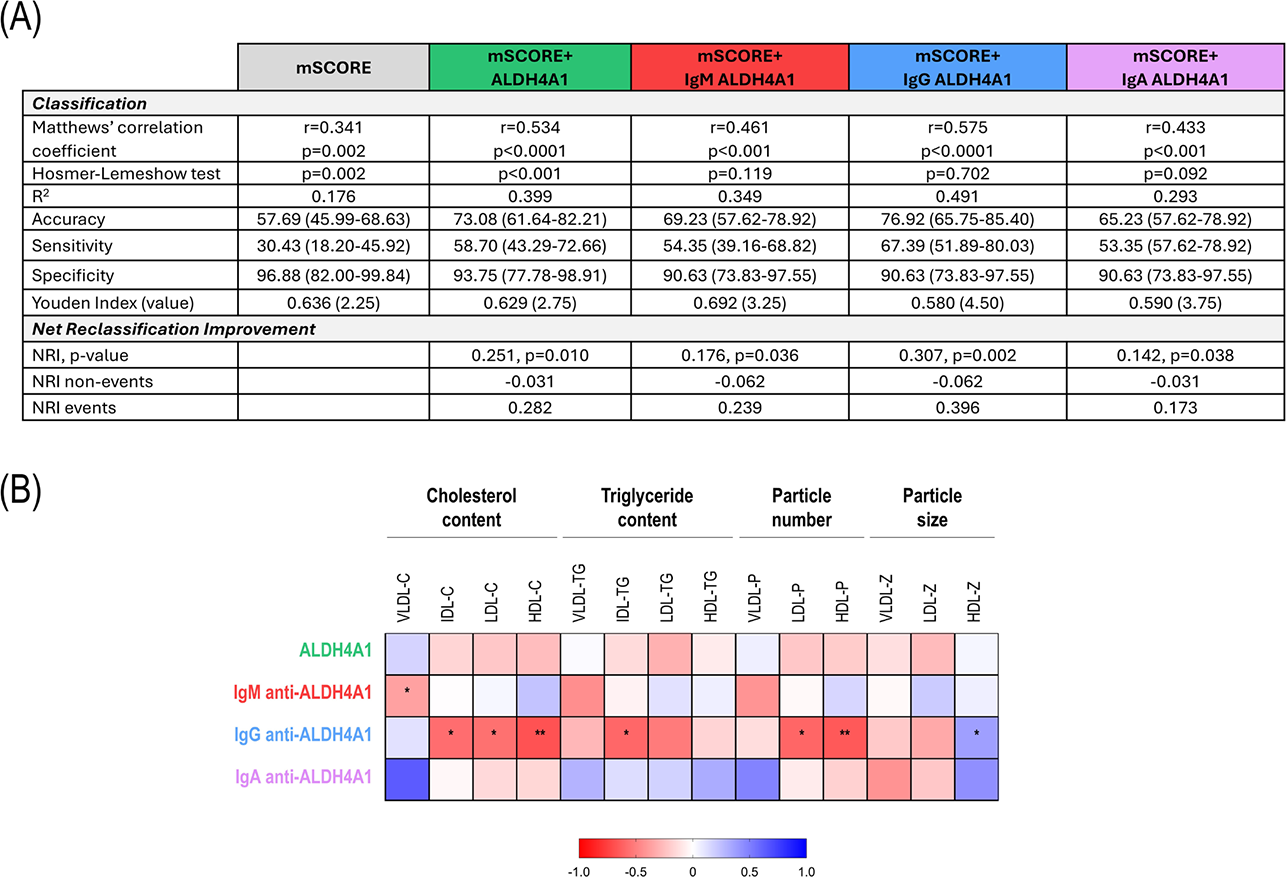
Results: ALDH4A1 serum levels did not differ between RA, CSA and controls (p=0.354). Reduced anti-ALDH4A1 antibodies (IgM: p=0.008, IgG: p=0.011, IgA: p=0.018) were found in arthritis compared to controls. These findings were confirmed in the validation cohort (ALDH4A1: p=0.981, IgM: p=0.012, IgG: p=0.009, IgA: p=0.048). ALDH4A1 serum levels were associated with 32 protein hits (protein-protein interaction: p=5.8·10 -8 ) which informed functional apoptotic-related proteomic pathways (Figure 1A), cell-free DNA (nDNA: r=0.305, p=0.005; mtDNA: r=0.103, p=0.358), and eicosanoid-related lipidomic signatures in early arthritis (Figure 1B) linked to arachidonic acid metabolism, alpha-linolenic, eicosanoid and docosahexaenoic metabolic pathways (enrichment ratio>30 and p-value<0.010 in all cases); whereas a diverging pattern was noted for anti-ALDH4A1 antibodies. Correlation analyses revealed strong associations among isotypes in HC, whereas a progressive decline was noted towards CSA, recent-onset RA, and established RA groups (Figure 1C). IgG anti-ALDH4A1 exhibited protective associations with lipoprotein traits (VLDL, LDL and HDL particle content and number, all p<0.050) and cardiometabolic risk factors (namely dyslipemia, obesity, urate and hepatic transferases, all p<0.050), whereas no associations were observed for the rest of isotypes (IgM and IgA). IgG3 antibodies predominated IgG responses in patients and controls, and negatively correlate complement levels in RA (C3 and C4, both p<0.050). Increased ALDH4A1 (p<0.001) and reduced IgM (p=0.015) or IgG (p=0.009) anti-ALDH4A1 antibodies independently were associated with atherosclerosis in arthritis patients, although no effect was observed for IgA (p=0.996), and independent predictor effect confirmed in univariate and multivariate regression models (ALDH4A1: 1.678 [1.015 – 2.772], p=0.040; IgM anti-ALDH4A1: 0.840 [0.736 – 0.959], p=0.010; and IgG anti-ALDH4A1: 0.722 [0.565 – 0.923], p=0.006). The validation cohort confirmed these findings in relation to CV disease history (ALDH4A1: p=0.007, IgM: p=0.012; IgG anti-ALDH4A1: p=0.019; and IgA anti-ALDH4A1: p=0.879). Adding ALDH4A1 or IgM/G anti-ALDH4A1 antibodies improved risk stratification over SCORE, most notably for IgG, based on classification, diagnostic statistics and net reclassification improvement in recent-onset RA (Figure 2A). TNF blockade did not lead to changes in ALDH4A1 nor in antibody levels, whereas increases in IgG antibodies occurred in responders (p=0.040). ALDH4A1 tracked with TNF dynamics under TNF blockade (r=0.610, p=0.027), but not with clinical improvement (r=-0.071, p=0.817). Changes in IgG anti-ALDH4A1 paralleled changes in lipoprotein features (Figure 2B).
Conclusions: the ALDH4A1/anti-ALDH4A1 axis emerges as a novel player bridging lipid disturbances, autoimmunity and atherosclerosis along the whole arthritis spectrum. From a translational standpoint, these findings bridge molecular and clinical dimensions: elucidating functional pathways, improving risk prediction, and informing therapeutic strategies. This is the first evidence on the role of ALDH4A1 as an antigen in RMDs, hence highlighting the involvement of mitochondrial targets.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.