fetching data ... 
Background: Rheumatoid arthritis (RA) exhibits marked clinical and biological heterogeneity, contributing to substantial variability in treatment response, including therapies targeting T-cell activation.[1,2] This interpatient diversity limits the effectiveness of uniform T-cell–modulating therapies, as underlying immune dysregulation and T-cell–associated pathways differ across individuals. In the absence of reliable biomarkers to predict treatment efficacy, therapeutic decision making remains largely empirical, with clinical decisions dependent on trial-and-error approaches.
Objectives: To enable a precision medicine approach for predicting therapeutic response in RA, we developed and validated a biologically informed classifier. This molecular treatment response signature (MTRS) is specifically tailored to T-cell activation inhibition, and consequently, delivers higher response rates and avoids therapy in those with a low likelihood of response to T-cell activation inhibition for RA.
Methods: Blood-based multi-omics data, including transcriptomic profiles, SNP genotyping, baseline clinical characteristics, and treatment outcomes, were collected from multiple independent RA studies: an RA registry cohort (n = 340) and retrospective cohorts from three company–sponsored clinical trials (n = 219). Candidate predictors across transcriptomic and genetic features were screened and reduced using a structured feature reduction strategy. These features were used to develop a supervised machine-learning classifier trained to predict ACR50 response at 24 weeks. Classifier performance was evaluated using cross-validation in the training cohort and confirmed using an independent validation cohort.
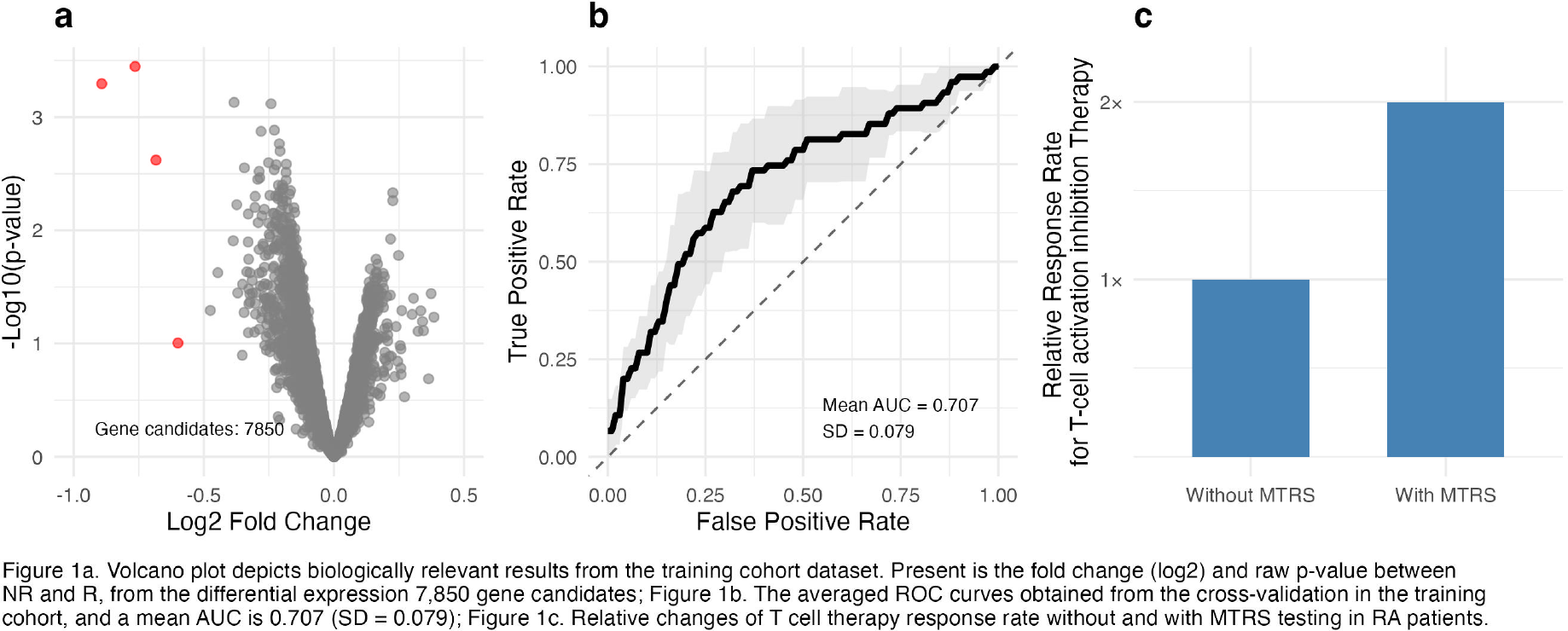
Results: Data collected from RA samples were divided into training (N = 360) and validation (N = 199) cohorts. Demographic and baseline clinical characteristics were largely comparable between cohorts (Table 1). A total of 7,850 gene expression profile (GEP) features were quantified by transcriptomic profiling. The volcano plot showed the magnitude of change and strength of statistical evidence utilizing the GEP between response vs. non-response groups, in which the cutoffs designated as 0.5 for log2 fold change and 0.1 for raw p-value (Figure 1a). A selected group of multi-omic features, coupled with patient baseline clinical parameters, were further incorporated into the development of the MTRS. The MTRS demonstrated strong overall predictive performance (Figure 1b). In cross-validation within the development cohort, the classifier achieved an AUC of 0.707 (SD = 0.079) for distinguishing non-responders from responders, clinically achieving ACR50. When evaluated in the independent validation cohort, the classifier achieved an AUC of 0.663 across RA populations. This supports an improved response rate in the selected cohort by 2x times (Figure 1c).
Conclusions: Here we describe the development and validation of a T-cell–specific MTRS for patients with rheumatoid arthritis. This T-cell MTRS enables accurate patient stratification for T-cell–targeted therapy, leading to improved clinical outcomes. In addition, this classifier enables more precise identification of appropriate patient populations for clinical trial enrollment and supports personalized treatment strategies aimed at achieving optimal therapeutic efficacy [3].
Baseline clinical characteristics
| Variable | Categories | Training (N = 360) | Validation (N = 199) | p-value |
|---|---|---|---|---|
| Age (mean (SD) | 58.88 (12.50) | 59.57 (13.29) | 0.543 | |
| Gender (n (%)) | Female | 295 (81.9) | 167 (83.9) | 0.636 |
| Male | 65 (18.1) | 32 (16.1) | ||
| Race (n (%)) | White | 312 (86.7) | 170 (85.4) | 0.279 |
| Other races | 46 (12.8) | 25 (12.6) | ||
| Unknown | 2 (0.6) | 4 (2.0) | ||
| BMI (mean (SD)) | 30.49 (6.92) | 30.95 (8.27) | 0.479 | |
| ACPA Binary (n (%)) | Negative | 138 (39.5) | 13 (56.8) | <0.001 |
| Positive | 211 (60.5) | 86 (43.2) | ||
| CDAI (mean (SD)) | 28.48 (11.86) | 31.02 (13.88) | 0.023 | |
| Tender joint counts (mean (SD)) | 10.72 (7.01) | 11.88 (8.28) | 0.08 | |
| Swollen joint count (mean (SD)) | 7.43 (5.06) | 7.20 (5.86) | 0.625 | |
| Biologic naïve (n (%)) | 70 (19.4) | 98 (49.2) | <0.001 |
Volcano plot, ROC curves and Relative response rate improvement
REFERENCES: [1] Weyand CM, McCarthy TG, Goronzy JJ. Correlation between disease phenotype and genetic heterogeneity in rheumatoid arthritis. J Clin Invest. 1995 May;95(5):2120-6.
[2] Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–2038.
[3] Pitzalis C, Choy EHS, Buch MH. Transforming clinical trials in rheumatology: towards patient-centric precision medicine. Nat Rev Rheumatol. 2020;16(10):590-599.
Acknowledgments: NIL.
Disclosure of Interests: Kunbin Qu Yes. The author has served as a consultant for Scipher Medicine., Lixia Zhang Yes. The author is an employee of Scipher Medicine., Angus Wong Yes. The author is an employee of Scipher Medicine., Alex Jones Yes. The author is an employee of Scipher Medicine., Sherry Guardiano Yes. The author is an employee of Scipher Medicine., Charles Younger Yes. The author is an employee of Scipher Medicine., Reginald Seeto Yes. The author is an employee of Scipher Medicine., Ryan Phan Yes. The author is an employee of Scipher Medicine.