fetching data ... 
Background: Real-world evidence derived from administrative health data is essential for understanding the long-term economic and clinical impacts of Rheumatoid Arthritis (RA) treatments. However, such studies are frequently plagued by confounding by indication: patients with higher disease activity are prescribed higher doses of Glucocorticoids (GC), and these same patients independently incur higher healthcare costs due to disease severity. Standard statistical methods fail to correct this bias when key confounders, such as disease activity, are missing from administrative data. While Instrumental Variable (IV) methods can correct for unmeasured confounding, valid instruments are rarely available in clinical datasets, forcing researchers to draw biased estimates. There is a critical need for accessible IV-free analytic tools that can reliably estimate causal effects in observational studies.
Objectives: To develop a novel IV-free causal inference framework (2sCOPE-MDN) that integrates a flexible Artificial Intelligence (AI) framework with Copula theory to correct for unmeasured confounding. We aimed to demonstrate its clinical utility by estimating the causal impact of systemic Glucocorticoid dosage on annual healthcare costs in a population-based cohort of incident RA patients. The results are validated against a gold-standard physician-preference IV design.
Methods: Data Source: We conducted a population-based retrospective cohort study using comprehensive health administrative data from Population Data BC (British Columbia, Canada). The dataset captures all provincially funded healthcare services (1995–2024), including physician visits, hospitalizations, and all dispensed outpatient medications, ensuring complete population coverage without selection bias.
Study Population: We identified incident RA patients using a validated algorithm requiring at least 2 RA diagnosis codes and 2 months apart, and a 5-year washout period.
The AI-Driven Causal Framework (2sCOPE-MDN): We addressed unmeasured confounding by indication using a two-stage approach. First, in the AI Estimation Stage, we trained a Mixture Density Network (MDN) to model the complex conditional distribution of GC dosing based on high-dimensional baseline covariates. Unlike traditional regression, this neural network flexibly captures non-linear prescribing relationships. Second, in the Causal Correction Stage, we utilized the MDN output to apply a Gaussian Copula transformation, generating a “control function.” This function captures the correlation between GC exposure and unobserved error terms (e.g., unmeasured disease severity), effectively disentangling variation driven by clinical indication from true causal variation.
Validation: We compared our method against naive Ordinary Least Squares (OLS) regression (prone to unmeasured confounding bias) and a benchmark correction method using physician prescribing preference as IV, a gold standard for controlling unmeasured confounding.
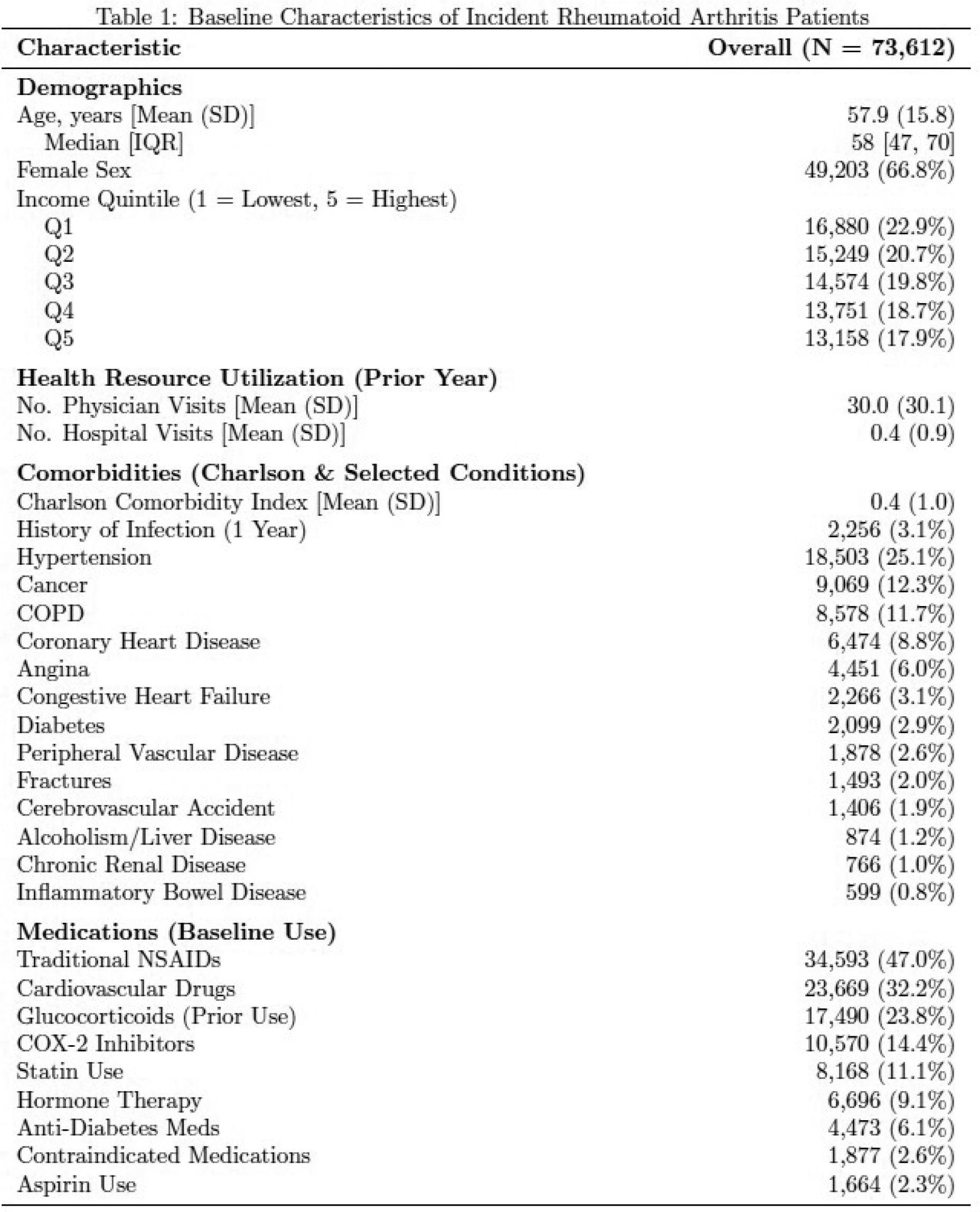
Results: Baseline Characteristics (Table 1): The cohort included 73,612 incident RA patients with a mean follow-up of 12.1 years. The mean age at diagnosis was 57.9 years (SD: 15.8), and 66.8% were female. The cohort exhibited a significant burden of comorbidities and healthcare utilization in the year prior to diagnosis, including hypertension (25.1%), cancer history (12.3%), COPD (11.7%), and a mean of 30.0 physician visits (SD: 30.1). Notably, 23.8% of patients had prior glucocorticoid exposure before the index date.
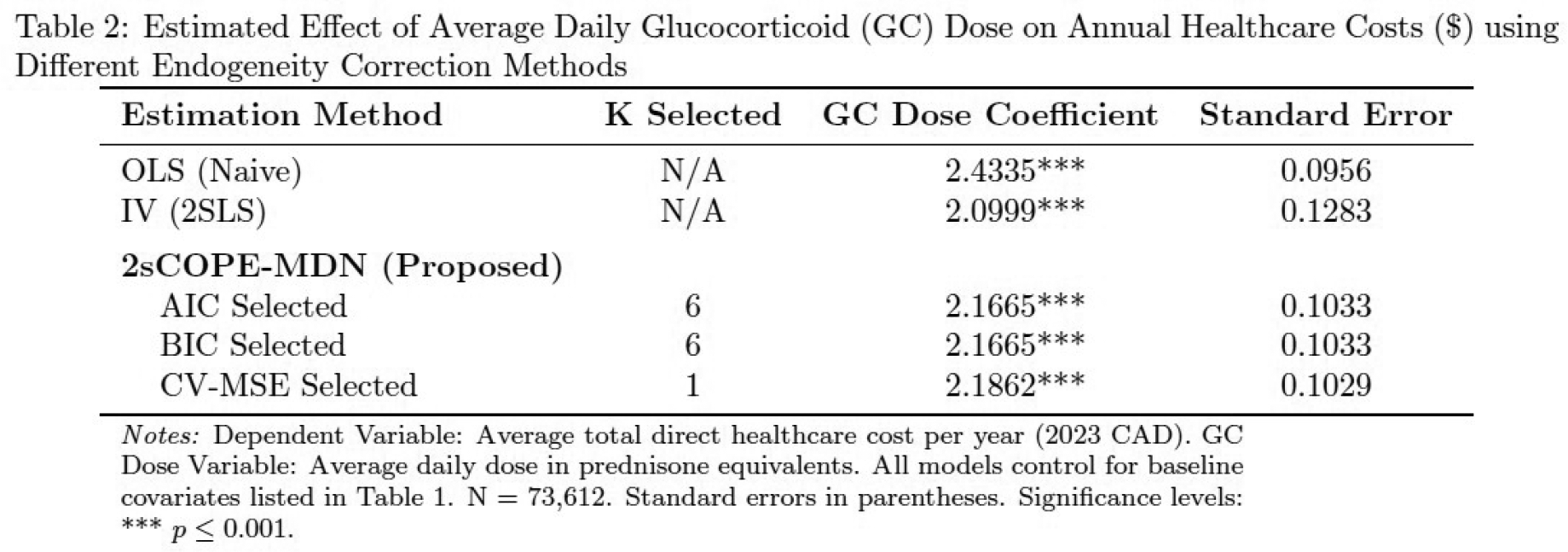
Causal Effect Estimates (Table 2): OLS estimated that each 1 mg unit increase in average daily GC dose increased annual healthcare costs by $2.43 (SE: 0.10); this estimate is likely inflated, incorrectly attributing costs driven by unmeasured disease severity to the medication itself. In contrast, the benchmark physician-preference IV model, which effectively controls for unmeasured confounding, estimated a lower true causal cost of $2.10 (SE: 0.13). Crucially, our proposed AI-driven 2sCOPE-MDN method corrected the OLS bias, yielding an estimate of $2.17 (SE: 0.10). This result aligns closely with the IV benchmark while offering greater precision through smaller standard errors without requiring IV. Furthermore, the method proved robust across different model selection criteria (AIC, BIC, Cross-Validation), consistently producing estimates between $2.16 and $2.19, demonstrating that the model effectively disentangled the treatment effect from the background noise of patient severity.
Conclusions: We present 2sCOPE-MDN, a robust and accessible AI-Driven analytical tool that allows rheumatology researchers to derive reliable causal estimates from observational data, even when critical confounders like disease activity are unmeasured. Crucially, this method replicates the rigor of an Instrumental Variable (IV) design without requiring an external instrument and therefore removes the most significant barrier to causal inference, where valid instruments are notoriously difficult to identify. This framework democratizes causal inference for administrative data research and offers a powerful alternative for comparative effectiveness and cost-of-illness studies in the frequent scenarios where RCTs are impractical and valid instruments are unavailable.
REFERENCES: [1] Guidelines for the Economic Evaluation of Health Technologies: Canada (4th Edition).
[2] Joshua D. Angrist and Alan B. Krueger. 1991. Does Compulsory School Attendance Affect Schooling and Earnings? The Quarterly Journal of Economics 106, 4 (1991), 979–1014. Publisher: Oxford University Press.
[3] Joshua D. Angrist and Jörn-Steffen Pischke. 2009. Mostly Harmless Econometrics: An Empiricist’s Companion . Princeton University Press.
[4] Jörg Breitung, Alexander Mayer, and Dominik Wied. 2023. Asymptotic Properties of Endogeneity Corrections Using Nonlinear Transformations. arXiv:2207.09246 [econ].
Acknowledgments: NIL.
Disclosure of Interests: None declared.