fetching data ... 
Background: Rheumatoid arthritis (RA) is an autoimmune disease characterized by inflammation of the joint synovial tissue. Despite a broad array of treatment options, only 1/3 of patients adequately respond to any given therapy, indicating a substantial need for methods to personalize treatment choice and predict treatment response [1]. Synovial pathotypes, classified by histological staining based on cell type abundance within the synovium, are a potential route for personalized treatment. Several studies have demonstrated potential for treatment stratification based on synovial characteristics, which are usually divided into myeloid, lymphoid or fibroid-predominant patterns. Previous work has established that pathotypes are differentiable at a transcriptome-wide level, suggesting that gene expression patterns differ across pathotypes [2]. However, pathotyping of synovial biopsies remains invasive, costly, and requires specific expertise for histological grading. The development of a non-invasive, peripheral blood transcriptomic classifier of synovial pathotypes could substantially improve treatment assignment and overall outcomes in RA.
Objectives: To non-invasively identify pathotypes in blood and synovium of patients with RA.
Methods: We collected bulk RNA-seq data from the Pathobiology of Early Arthritis Cohort (PEAC) in matched samples of blood and synovial tissue [2]. We used single-cell gene expression from Sun et. al [3]. to create the reference matrices for cell types in synovial tissue. To create a mixed cell type reference, we used quantile normalization of a standard blood cell reference dataset [4] and the pseudobulked synovial cell expression, enabling simultaneous estimation of fractions of cells originating from both compartments. We used the Gene Expression Deconvolution Interactive Tool [5] to perform cellular deconvolution. For each cell type, we computed a normalized abundance score by standardizing the estimated cell type fractions. To compare cell scores in blood between synovial pathotypes, we used non-parametric Wilcoxon tests. To assess discrimination of pathotypes by cell scores, we fit regression models for classification of each pathotype using LASSO regression [6]. To validate the relevance of our mixed cell type scoring method in quantifying synovial characteristics, we computed scores as described above, using bulk RNA-seq measured from synovial samples in the same patients. Individual synovial cell types were compared between pathotypes using Wilcoxon tests. Overall cell type scores for erythrocytes and chondrocytes were used as tissue-specific controls to validate expected abundance in synovium and blood.
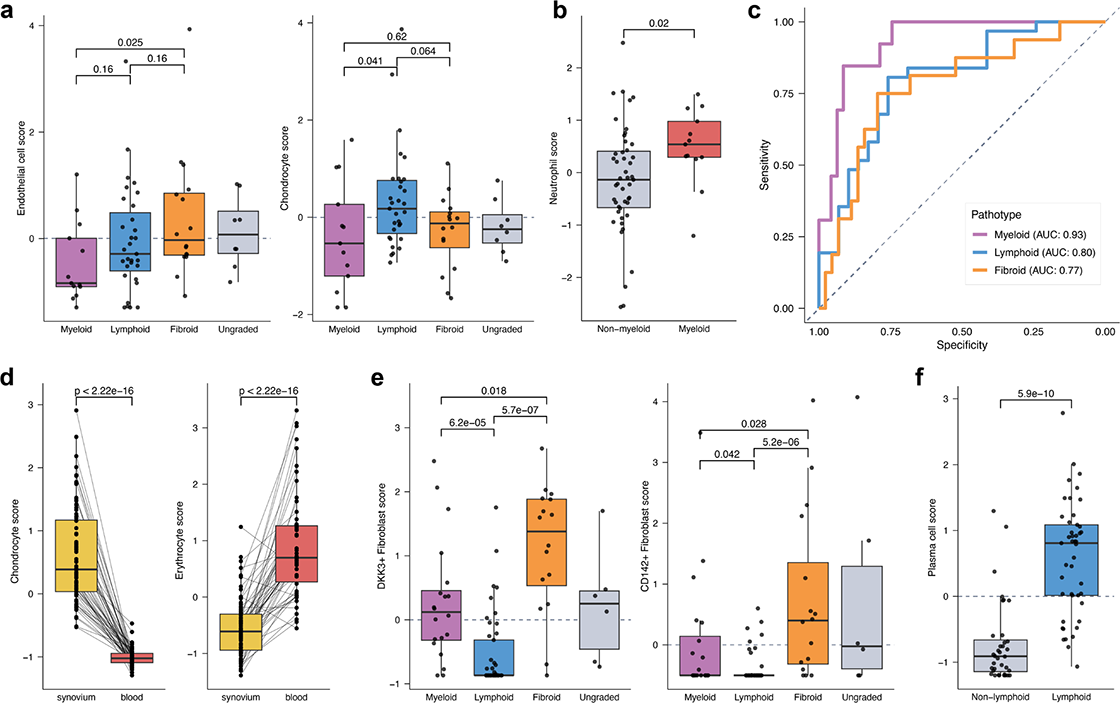
Results: Mixed cell type deconvolution estimated small fractions of synovial cell RNA in peripheral blood. Several cell type scores derived from synovial cells were measurable in blood and significantly associated with pathotype (Figure 1A). Most notably, estimated cell type scores of granulocytes were significantly different in patients with a myeloid pathotype, including neutrophils (Figure 1B).
Small sets of cell types identified by LASSO regression could discriminate synovial pathotypes in blood with high accuracy (Figure 1C). Myeloid pathotypes were most readily discriminated (AUC 0.93 [95% CI: 0.87-0.99]), while also lymphoid (AUC 0.80 [95% CI: 0.69-0.91]) and fibroid (AUC 0.77 [95% CI: 0.63-0.91]) pathotypes had moderate but clinically useful discrimination. We observed significant differences in positive controls for erythrocyte and chondrocyte scores between blood and synovium, suggesting relevant quantification of cell type abundance using our mixed deconvolution method (Figure 1D). Several cell type scores in synovial samples were also differentially abundant across pathotypes, including elevation of DKK3 + and CD142 + fibroblast scores in the fibroid pathotype (Figure 1E). Notably, we also observed elevation of plasma cell scores in the lymphoid pathotype, consistent with the results described in Lewis et. al. (Figure 1F).
Conclusions: We demonstrate discrimination of synovial pathotypes non-invasively using deconvolution of peripheral blood RNA-seq data. Pathotypes could be discriminated using scores from a parsimonious set of cell types. Furthermore, these cell types were logically related to the pathotype being classified (for example, granulocytes were implicated in discrimination of the myeloid pathotype). Deconvolution of synovial tissue RNA-seq further identified differences in cell type scores between pathotypes, consistent with previously described differences in gene expression. Differential cell type scores in both blood and synovium were largely relevant to known pathotype characteristics. Validation using a larger cohort of rheumatoid arthritis patients with known synovial pathotypes and blood samples is needed to confirm the utility of mixed deconvolution in non-invasive classification. Overall, our work presents a novel approach to non-invasive resolution of synovial characteristics, opening the door to guide individualized treatment decisions in rheumatoid arthritis.
REFERENCES: [1] Winthrop, Kevin L et al. “Chasing the target: reports from the Advances in Targeted Therapies meeting, 2024.” Annals of the rheumatic diseases 84,6 (2025)
[2] Lewis, Myles J., et al. “Molecular portraits of early rheumatoid arthritis identify clinical and treatment response phenotypes.” Cell reports (2019)
[3] Sun, Hao et al. “CD142-positive synovial fibroblasts drive meniscus destruction in rheumatoid arthritis.” Nature communications 16,1 6942. 28 Jul. 2025.
[4] Tabula Sapiens Consortium* et al. “The Tabula Sapiens: A multiple-organ, single-cell transcriptomic atlas of humans.” Science (New York, N.Y. ) 376,6594 (2022)
[5] Nadel, Brian B et al. “The Gene Expression Deconvolution Interactive Tool (GEDIT): accurate cell type quantification from gene expression data.” GigaScience 10,2 (2021)
[6] Friedman J, Hastie T, Tibshirani R (2010). “Regularization Paths for Generalized Linear Models via Coordinate Descent.” Journal of Statistical Software , 33 (1), 1-22.
Acknowledgments: NIL.
Disclosure of Interests: Clove Taylor: None declared, Andreas Kerschbaumer Galapagos, JNJ, MSD, Novartis, Pfizer, Stada, UCB, AbbVie, Lilly, JNJ, UCB, Andrew Moore: None declared, Purvesh Khatri Inflammatix, Inc., Inflammatix, Inc.