fetching data ... 
Background: Difficult-to-treat (D2T) rheumatoid arthritis (RA) represents a high burden condition with high socioeconomic costs and reduced quality of life. While approximately 20% of patients fail multiple biologics and targeted synthetic disease-modifying anti-rheumatic drugs (b/ts DMARDs), the underlying pathological mechanisms remain unclear. A major challenge in D2T-RA is distinguishing true biological refractoriness from non-inflammatory contributors (e.g. pain, comorbidities). To date, the synovial tissue features of D2T-RA remain largely unexplored.
Objectives: To characterise the histological and molecular features of synovial tissue in D2T-RA patients, specifically assessing the presence of active synovial inflammation.
Methods: Patients with RA fulfilling the EULAR D2T-RA criteria were recruited at QMUL. Clinical data were collected, and synovial biopsy of a clinically active swollen joint was performed. Synovial biopsies were stained for immune cell markers, and quantitative scores were calculated; biopsies were classified into three distinct pathotypes (lympho-myeloid, diffuse-myeloid, and pauci-immune) based on the degree of immune cell infiltration and synovitis. Synovium bulk RNA was sequenced with Nanostring nCounter using a custom synovium-specific 500 gene. Additionally, clinical data and baseline synovial biopsies from responders to the 1 st line treatment from the biopsy-driven Stratification of Biologic Therapies for RA by Pathobiology (STRAP) randomised controlled trial were assessed as comparators.
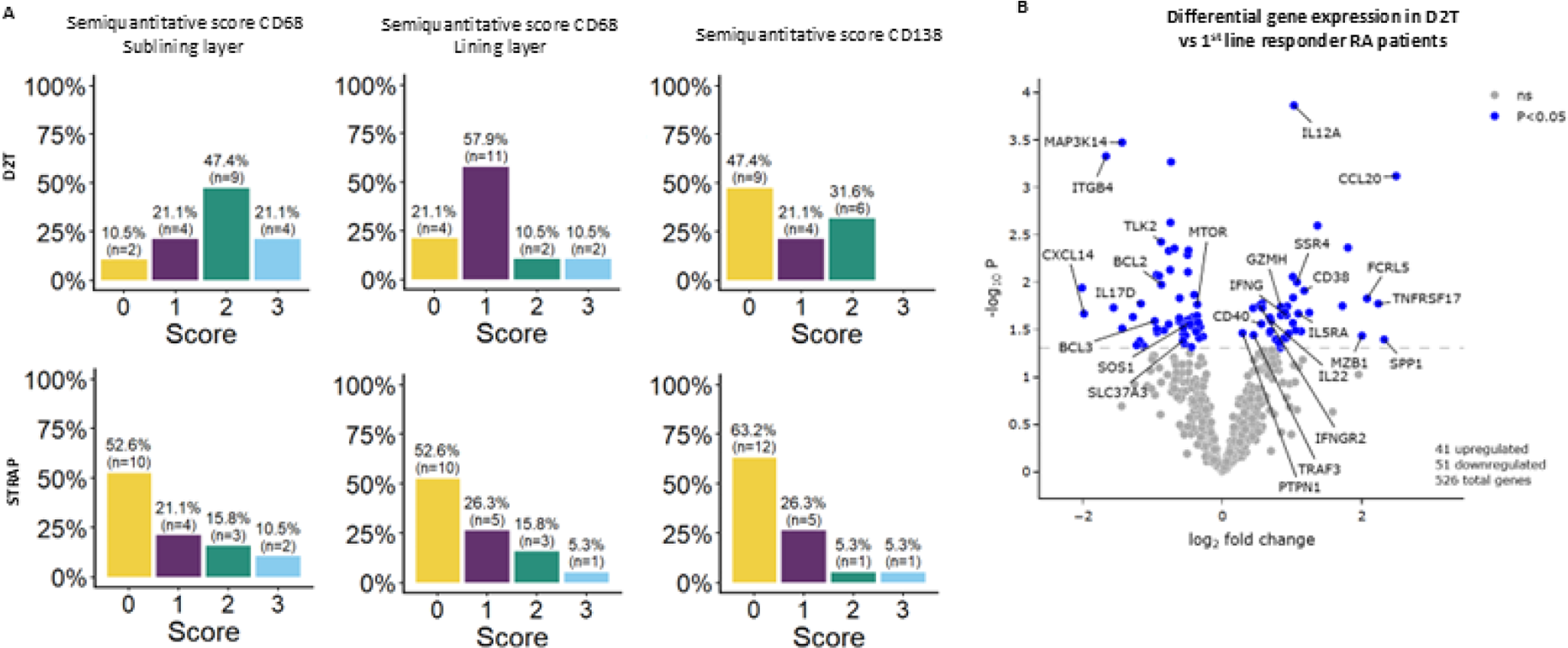
Results: Twenty-one D2T-RA patients were included, with a median disease duration of 130 months (87-230). Nineteen age-, sex- and synovial pathotype-matched established RA patients who responded to the 1 st line treatment with bDMARD in the STRAP trial were included as comparators. Crucially, all D2T patients presented with high disease activity and confirmed clinical synovitis (high DAS28-CRP, tender joint counts, swollen joint counts, and high synovial thickness by ultrasound; Table 1). 62% (n=13) of participants failed ≥3 b/ts DMARDs, and 71.4% (n=15) were under concomitant glucocorticoid treatment. Importantly, none of the patients had major overlapping chronic pain, with limited presence of concomitant cardiovascular or other systemic diseases (i.e. hypertension, diabetes). Overall, clinical features of D2T-RA patients were comparable with matched responders (Table 1). Histologically, 42,9% (n=9) of D2T synovium was classified as diffuse-myeloid. Higher macrophages sublining scores were observed compared to 1 st line responders (Figure 1A). Sublining CD68 scores positively correlated with the pre-biopsy synovial power doppler (PD) at baseline. Comparing Nanostring nCounter data of D2T patients (n=17) and 1 st line responders (n=19), we identified 41 upregulated and 51 downregulated genes in D2T RA patients (Figure 1B), including several plasma cell genes (CD38, MZB1, SSR4). We also observed significant upregulation of SPP1, a marker of inflammatory macrophages in the synovium. Accordingly, we observed an upregulation of pathways associated with inflammatory response, such as interferon-γ, complement pathway and neutrophil degranulation response, and downregulation of pathways associated with several Fibroblast Growth Factor Receptor (FGFR) signalling.
Conclusions: This study provides the first histological and molecular characterisation of synovial tissue in D2T-RA. Our results demonstrate that D2T-RA represents a state of true biological refractoriness driven by active histological synovitis and concurrent innate and adaptive immune activation. While acknowledging the selection bias inherent to a biopsy-driven cohort restricted to clinically and ultrasound active joints, identifying this specific biological endotype linked to refractoriness provides the molecular rationale for the Multi-drug resistant RA EU consortium to comprehensively dissect the intrinsic biological drivers of resistance versus extrinsic disease contributors.
Baseline characteristics of RA and D2T RA patients. Data reported as n (%) or median [IQR].
| 1
st
line responders
| D2T-RA (n=21) | |
|---|---|---|
| Gender female | 17 (89.5%) | 18 (85.7%) |
| Age | 55 (42-62) | 54 (41-59) |
| Disease duration in months | 36 (12-84) | 130 (87-230) |
| ACPA positivity | 13 (68.4%) | 12 (57.1%) |
| RF positivity | 12 (63.2%) | 15 (71.4%) |
| Tender joint count | 14 (9.5-18) | 15 (8.0-20) |
| Swollen joint count | 10 (9.0-11) | 7.0 (4.0-11) |
| VAS pain | 71 (58-86) | 74 (61-87) |
| CRP | 10 (3.5-22) | 9.0 (3.0-26) |
| DAS28-CRP | 6.1 (5.5-6.6) | 5.6 (5.2-6.7) |
| Synovial Thickness | 2.0 (2.0-3.0) | 2.0 (2.0-3.0) |
| Power Doppler | 2.0 (1.0-2.0) | 1.0 (0.0-1.0) |
| Synovitis score | ||
| No synovitis (0–1) | 2 (10.5%) | 3 (14.3%) |
| Low synovitis (2–4) | 10 (52.6%) | 11 (52.4%) |
| High synovitis (5–9) | 7 (36.8%) | 5 (23.8%) |
| Pathotype | ||
| Diffuse-Myeloid | 9 (47.4%) | 9 (42,9%) |
| Lympho-Myeloid | 5 (26.3%) | 5 (23.8%) |
| Pauci-immune | 5 (26.3%) | 5 (23.8%) |
Score distribution of positive CD68 and CD138 cells within study cohorts and differential gene expression in D2T vs 1 st line responders. Score distribution of lining and sublining CD68 and CD138 cells in D2T and 1 st line responders (A). Differentially expressed genes between D2T and 1 st line responders; significant genes are in blue, non-significant genes in grey (B).
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.