fetching data ... 
Background: Rheumatoid arthritis (RA) is a systemic autoimmune inflammatory disease characterized by chronic synovitis and progressive cartilage and bone destruction, leading to increased morbidity and mortality [1]. Approximately 30% of patients with RA develop osteoporosis involving the spine or total hip [2]. RA affects 0.5–1.0% of the general population and imposes substantial familial and socioeconomic burdens [3]. Despite advances in biologic and targeted synthetic disease-modifying therapies, nearly 20% of patients fail to achieve remission or sustained low disease activity [4, 5]. Consequently, RA continues to severely impair quality of life, increase disability risk, and reduce life expectancy, contributing to escalating healthcare costs [6]. Increasing evidence indicates that RA is a heterogeneous disorder characterized by diverse clinical phenotypes, variable genetic susceptibility, and non-uniform immune responses [7]. Rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibodies (ACPAs) are the principal serological biomarkers for RA and define seropositive RA (SpRA). ACPAs detected by the anti-cyclic citrullinated peptide (anti-CCP) assay included in RA classification criteria demonstrate high specificity and moderate sensitivity, with reduced performance in early disease [8, 9]. In contrast, patients lacking both RF and ACPAs are classified as having seronegative RA (SnRA). SnRA presents challenges in early diagnosis and heterogeneous treatment responses and may represent a distinct disease subset with divergent immunopathological mechanisms.
Objectives: Early diagnosis of seronegative rheumatoid arthritis (SnRA) is often challenging due to lack of reliable immune markers. The aim of this study was to explore immunocyte phenotype of SnRA and identify their potential as therapeutic targets.
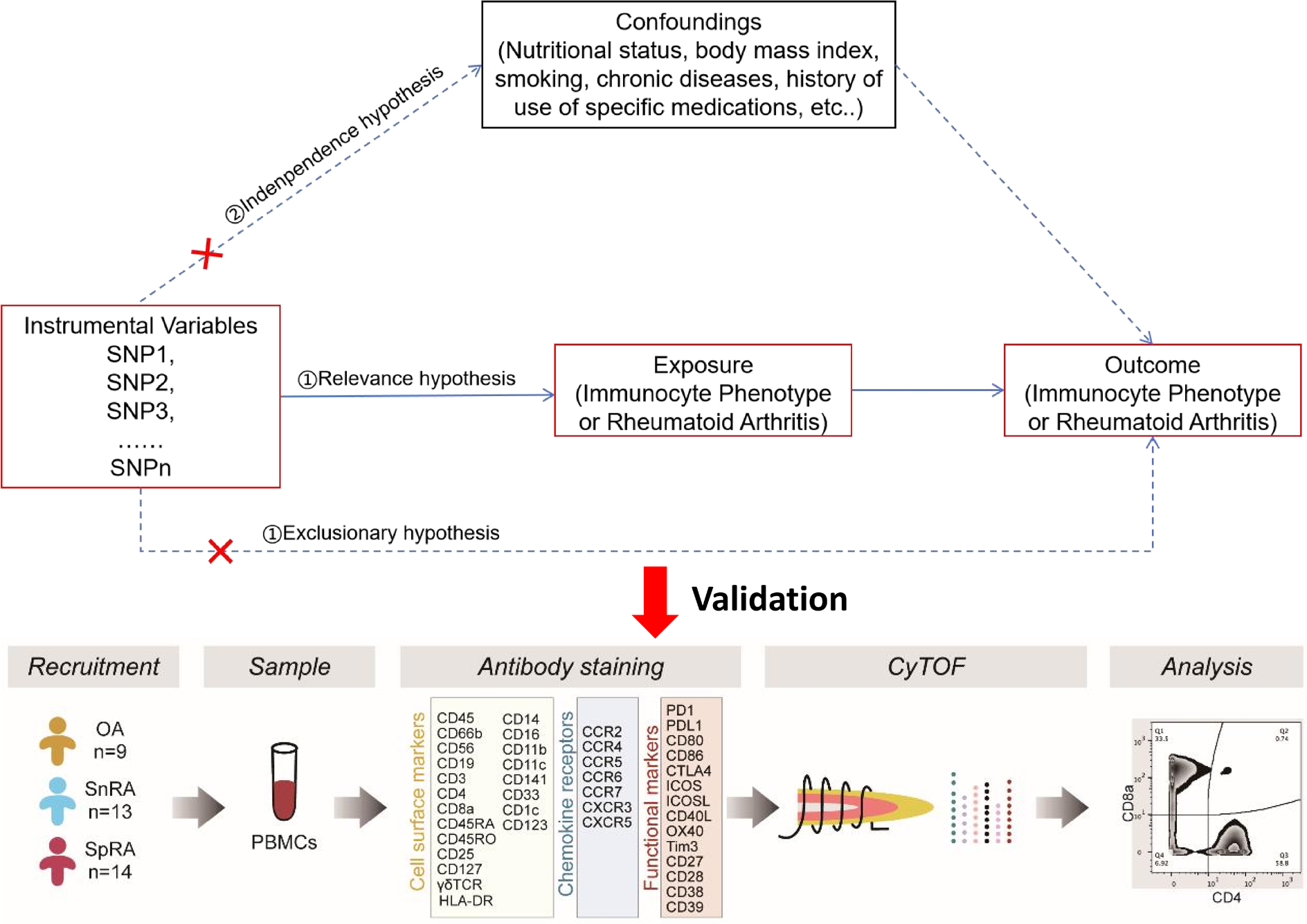
Methods: In this study, we performed a comprehensive analysis of causal immune cell traits associated with both SnRA and SpRA using a bidirectional two-sample Mendelian randomization (MR) design. We integrated genome-wide data from the FinnGen and OPEN GWAS repositories, and employed single-cell mass cytometry (CyTOF) to validate immune phenotypes distinguishing SnRA from seropositive RA (SpRA) and osteoarthritis (OA).
Results: Forward MR identified reduced HLA-DR expression on five myeloid subsets—including CD14 + monocytes, dendritic cells, and plasmacytoid DCs—as causally linked to SnRA, suggesting impaired antigen presentation. In contrast, stronger associations in SpRA indicated a greater reliance on adaptive immunity. This study included 9 OA, 13 SnRA, 14 SpRA patients. CyTOF validated diminished HLA-DR levels in SnRA myeloid cells and revealed innate immune shifts marked by expansion of CCR2 + CD33 + CD38 + monocytes and CCR2 + CD33 + CD38 + HLA-DR br DCs, driven by the CCL18–CCR2 axis. These cells effectively distinguished SnRA from SpRA and OA, supporting their role as diagnostic biomarkers.
Conclusions: Our findings reveal distinct immune features and therapeutic targets in SnRA, advancing precision approaches for this understudied RA subtype.
Flow chart of the study design
REFERENCES: [1] Luo P, Gao FQ, Sun W, Li JY, Wang C, Zhang QY, et al. Activatable fluorescent probes for imaging and diagnosis of rheumatoid arthritis. Mil Med Res. 2023;10(1):31.
[2] Hauser B, Riches PL, Wilson JF, Horne AE, Ralston SH. Prevalence and clinical prediction of osteoporosis in a contemporary cohort of patients with rheumatoid arthritis. Rheumatology (Oxford). 2014;53(10):1759-66.
[3] Gibofsky A. Overview of epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis. Am J Manag Care. 2012;18(13 Suppl):S295-302.
[4] Yap HY, Tee SZ, Wong MM, Chow SK, Peh SC, Teow SY. Pathogenic Role of Immune Cells in Rheumatoid Arthritis: Implications in Clinical Treatment and Biomarker Development. Cells. 2018;7(10).
[5] Mok A, Rhead B, Holingue C, Shao X, Quach HL, Quach D, et al. Hypomethylation of CYP2E1 and DUSP22 Promoters Associated With Disease Activity and Erosive Disease Among Rheumatoid Arthritis Patients. Arthritis Rheumatol. 2018;70(4):528-36.
[6] van Esveld L, Cox JM, Kuijper TM, Bosch TM, Weel-Koenders AE. Cost-utility analysis of tapering strategies of biologicals in rheumatoid arthritis patients in the Netherlands. Ann Rheum Dis. 2023.
[7] Nakajima S, Tsuchiya H, Ota M, Ogawa M, Yamada S, Yoshida R, et al. Synovial Tissue Heterogeneity in Japanese Patients with Rheumatoid Arthritis Elucidated Using a Cell-Type Deconvolution Approach. Arthritis Rheumatol. 2023.
[8] Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, 3rd, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569-81.
[9] He Y, Lin J, Tang J, Yu Z, Ou Q, Lin J. iTRAQ-based proteomic analysis of differentially expressed proteins in sera of seronegative and seropositive rheumatoid arthritis patients. J Clin Lab Anal. 2022;36(1):e24133.
Acknowledgments: NIL.
Disclosure of Interests: None declared.