fetching data ... 
Background: The pathogenesis of Sjögren’s disease (SjD) and especially deterioration of ductal structures within the salivary glands of patients are underexplored. Lymphocytic infiltrations are a common histopathologic feature of SjD salivary glands and can be accompanied by the formation of lymphoepithelial lesions (LEL). LELs are defined by the presence of intraepithelial lymphocytes together with hyperplasia of basal ductal cells[1,2]. Different severity stages of LEL can be defined based on the degree of hyperplasia[3,4]. Increasing abundance of B-lymphocytes could be observed with higher severity of LELs. The presence of LELs is associated with various SjD features like disease activity scores, increased serum IgG and rheumatoid factor levels [3]. Salivary glands harbor physiologically numerous IgA antibody-secreting cells (ASCs) in all individuals. In SjD patients, also increasing numbers of autoreactive IgG/IgM plasma cells can be present [5]. SjD patients with a higher focus score display higher frequencies of salivary gland ASCs [6] indicating a link between ASCs and tissue pathology. However, little is known about ASCs abundance and phenotype in the context of LELs.
Objectives: Utilizing imaging mass cytometry (IMC), we assessed the abundance and phenotype of ASCs in salivary gland biopsies of SjD patients with different stages of LEL severity.
Methods: Formalin-fixed paraffin embedded tissues from 5 labial and 15 parotid salivary gland biopsies showing at least one LEL were selected from 17 SjD patients, with paired biopsies available from 3 patients. All SjD patients were female, positive for SSA antibodies, older than 18 years of age and fulfilled the ACR-EULAR classification criteria for SjD. The focus score, presence of germinal centers and severity of LELs were evaluated on Hematoxylin and Eosin stained sections. For each biopsy, a consecutive tissue section was used for staining and IMC acquisition using the Hyperion imaging system. A metal-conjugated antibody panel for broad immune phenotyping was applied including the markers CD138, Ki67, CD20, CD56, CD45 and IgG, amongst others. A total of 71 regions of interest (ROI) with different stages of LEL severity were defined across all 20 biopsies and quantified for the expression of named markers using the Visiopharm Integrater System. Abundance and phenotype of all ASCs within the ROIs was investigated in relation to disease features like ESSDAI, focus score, presence of germinal centers, stage of LELs and epithelial hyperplasia.
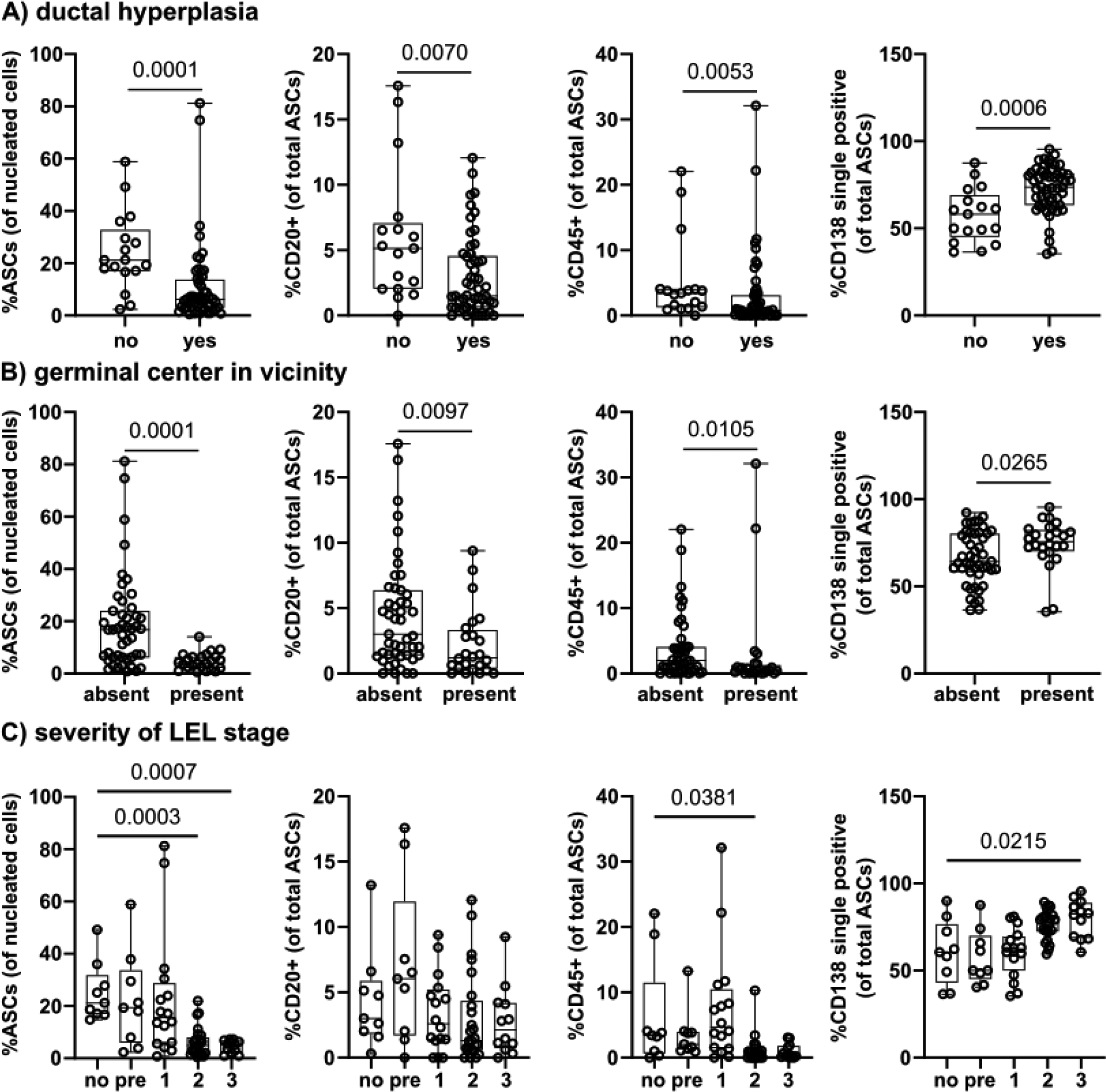
Results: The overall frequency of CD138+ salivary gland ASCs, relative to all nucleated cells within the ROI, was significantly decreased in ROIs with hyperplasia versus ROIs without hyperplasia (p < 0.001). ASCs were especially less abundant in ROIs with LEL stage 2 (hyperplasia in ≥ 50% of the epithelial area) and stage 3 (full hyperplasia of the epithelial area without visible lumen). Additionally, ASC frequencies were also significantly lower in ROIs containing germinal centers (p < 0.001). To assess the ASC population in more detail, we determined the proportion of immature CD138+CD20+ cells or CD138+CD45+ cells and presumably mature CD138 single positive cells as frequency of all ASCs within the ROI. Similar to total ASC frequencies, also the proportions of ASCs expressing CD20 or CD45 were significantly lower in ROIs with hyperplasia than ROIs without hyperplasia (p = 0.007 and p = 0.005, respectively). Also tendencies of reduced CD20+ and CD45+ ASC frequencies were observed with increasing severity of the LEL stage. On the contrary, likely more mature ASCs only positive for CD138 increased significantly in ROIs with hyperplasia (p < 0.001) and LEL stage 3 (p = 0.022). The same pattern of relatively less immature CD138+CD20+ and CD138+CD45+ ASCs but more mature CD138 single positive ASCs was observed dependent on the presence of germinal centers within the ROIs.
Conclusions: Overall, the frequency of ASCs among all nucleated cells decreased with progressing hyperplasia in salivary gland biopsies of SjD patients. This is potentially attributed to the expansion of the epithelium into the ductal lumen and the influx of B- and T-lymphocytes into the salivary gland in general, but also into the ducts itself. However, the less frequently appearing ASCs within the areas around the ducts are less often positive for CD20 and CD45, indicating a more mature ASC phenotype in the context of more severe LELs.
REFERENCES: [1] Ihrler, S., Zietz, C., Sendelhofert, A., Riederer, A. & Löhrs, U. Lymphoepithelial duct lesions in Sjögren-type sialadenitis. Virchows Arch. Int. J. Pathol. (1999).
[2] van Ginkel, M. S. et al. Presence of intraepithelial B-lymphocytes is associated with the formation of lymphoepithelial lesions in salivary glands of primary Sjögren’s syndrome patients. Clin. Exp. Rheumatol. (2019).
[3] van Ginkel, M. S. et al. Digital image analysis of intraepithelial B-lymphocytes to assess lymphoepithelial lesions in salivary glands of Sjögren’s syndrome patients. Rheumatology (2023).
[4] Delli, K. et al. Towards personalised treatment in primary Sjögren’s syndrome: baseline parotid histopathology predicts responsiveness to rituximab treatment. Ann. Rheum. Dis. (2016).
[5] Salomonsson, S. et al. Cellular basis of ectopic germinal center formation and autoantibody production in the target organ of patients with Sjögren’s syndrome: Ectopic Germinal Center Formation in Sjögren’s Syndrome. Arthritis Rheum. (2003).
[6] Szyszko, E. A. et al. Salivary glands of primary Sjogren’s syndrome patients express factors vital for plasma cell survival. Arthritis Res. Ther. (2011).
Acknowledgments: NIL.
Disclosure of Interests: None declared.