fetching data ... 
Background: Axial spondyloarthritis (axSpA) is a lifelong condition, with symptom onset most often between the ages of 20-30. The Royal National Hospital for Rheumatic Diseases (RNHRD), Bath has collected detailed clinical data on axSpA patients for over 4 decades, including individual patient phenotype, patient reported outcome measures (PROMs), imaging and serologic data. This vast quantity of health data is a valuable resource for understanding and predicting disease prognosis and response to treatment. Previous approaches to clustering of up to 5 years of data from the DESIR and Be-Giant early axSpA cohorts identified two distinct axSpA endotypes, with peripheral symptoms a predictor of poorer outcomes [1]. We aim to build on this work through harnessing a vast, real-world axSpA cohort to develop a novel AI clustering tool that can predict long-term (> 30 years) patient outcomes based on data captured in routine clinical practice.
Objectives: 1. To develop and demonstrate proof-of-concept for a novel clinical-aid decision tool that, by utilising PROMs and specified population features, provides the user (clinician) with subgroups of patients that can mathematically be classified as “similar”.
To use the resulting subgroups and their associated mean paths to predict the future disease trajectory of a patient, thereby providing a clinician with the opportunity to make decisions that positively influence the projected course of a patient’s trajectory.
This will enable, in future work, inference of influential disease, clinical or lifestyle traits from the subgroups, and quantification of the treatment effects of biologic DMARDs to aide in their optimal application.
Methods: We have developed a novel version of K-means clustering [2,3], that is well suited to longitudinal patient data. It is able to operate on data points (patients) that vary in their dimension (number of measurements), therefore enabling it to cluster patients by their provided medical records. For each cluster, the method also returns a “mean path” which the data in that cluster is synonymous with. This path provides a disease trajectory that describes the general trend for the associated cluster. The cluster and its mean path are the analytical tools leveraged by the method by which clinical insights and decisions can be made, including those outlined in the objectives.
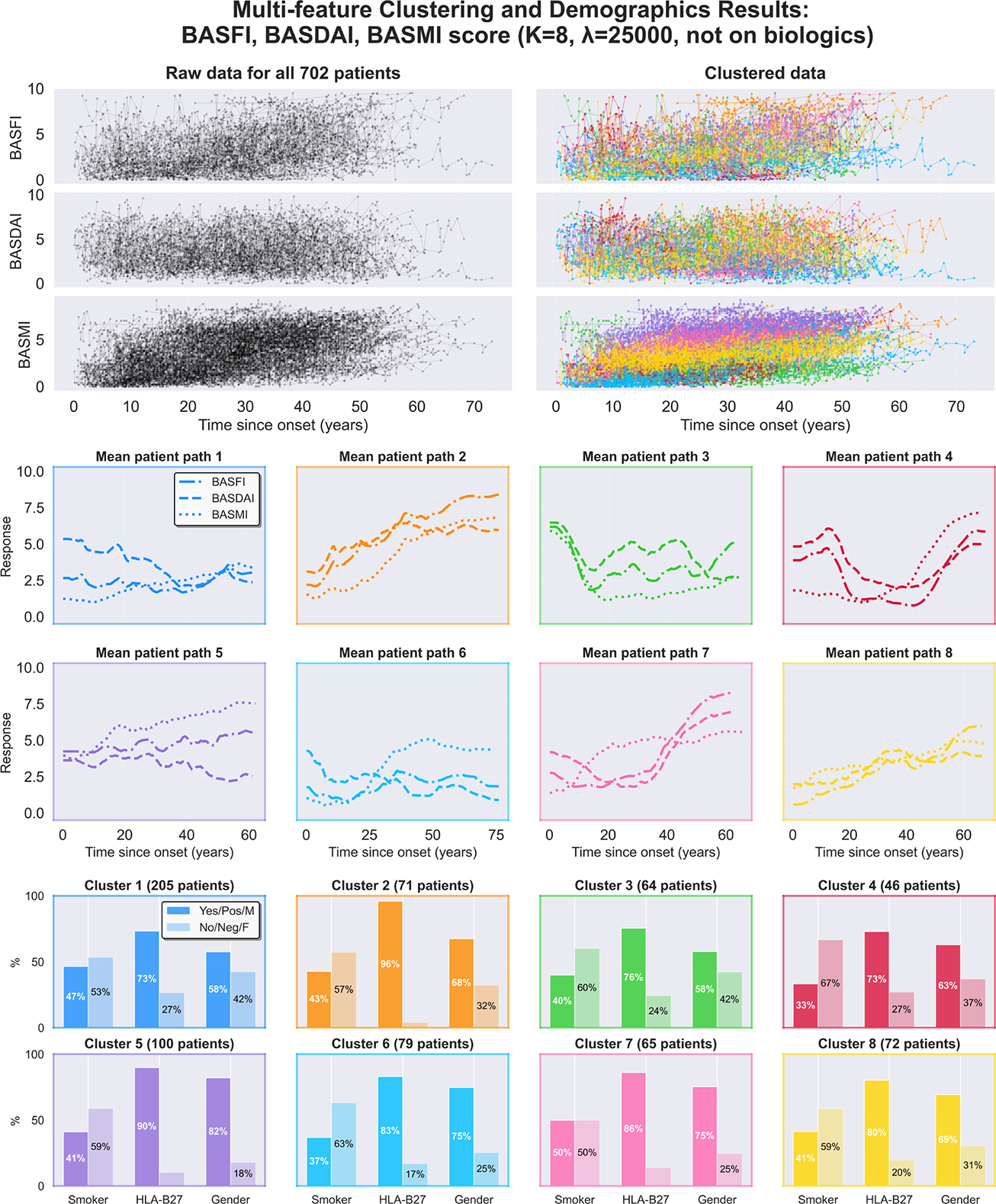
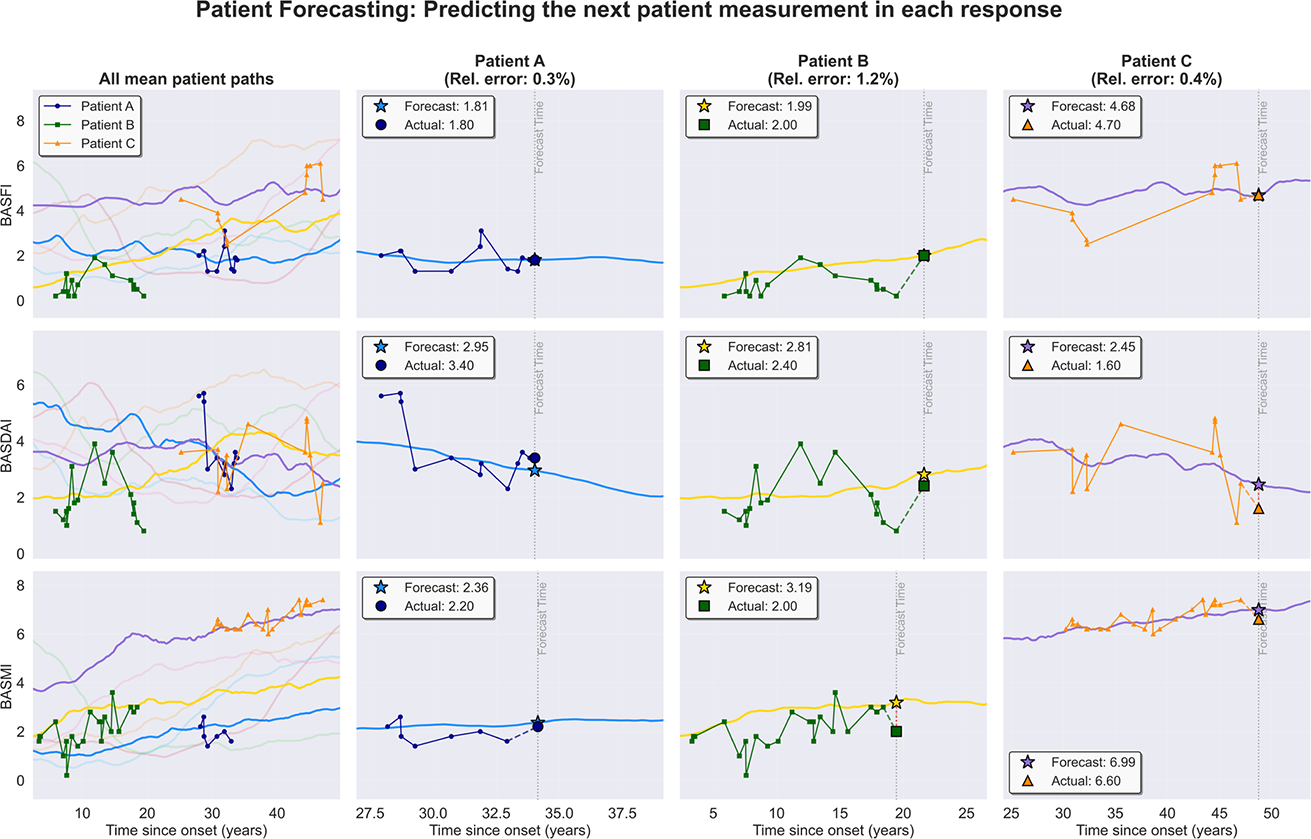
Results: Full functionality of the clustering tool was demonstrated via its ability to cluster on multiple responses from a population of 702 axSpA patients. Without any further processing, these clusters already allow the user to observe correlations between responses and to explore the demographics/clinical features behind a cluster of interest. We demonstrate this by running with a generic assignment of K=8 clusters on a subset of patients not on bDMARDS, thereby visualizing the natural history of the condition in terms of disease activity (BASDAI), function (BASMI), and spinal mobility (BASMI) (Figure 1). Similarity between the BASDAI and BASFI mean paths was observed, but not in BASMI. Specifically, across all clusters, the BASDAI and BASFI mean paths have the smallest time-average, centroid-average root mean square error (1.394 response measurement units), compared to BASFI vs BASMI (1.533 response measurement units) and BASDAI vs BASMI (2.132 response measurement units). The influence of HLA-B27 status, gender, and smoking status on the differing disease trajectories is also demonstrated in Figure 1. Post-clustering, we demonstrate the predictive capabilities of the tool. By assigning 3 selected patients to a mean path based on their historical BASFI, BASDAI and BASMI measures, we predict their next measurements in each response with 0.3%, 0.4% and 1.2% relative accuracy (i.e. their absolute predicted error as a proportion of their average training error); see Figure 2. Crucially, the value of this measurement is unknown to the tool; consistent with a real-world scenario of a clinician attempting to map the projected disease evolution for a particular patient. A key functionality of the clustering tool is the flexibility and adaptability to input different datasets for which clinical inferences/outputs can be determined. Clinicians can provide a data set and set the parameters for clustering; including the responses by which to cluster by, the chosen time variable (i.e. patient age, time since disease onset or time since diagnosis), and the number of clusters. This freedom of choice provides the user with a breadth of possibilities to explore but for which clinical knowledge is beneficial to configure the tool to unlock any potential hidden insights.
Conclusions: Through harnessing real-world axSpA data over four decades, we have developed an AI tool that can provide clinicians with patient subgroups that have similar disease trajectories. These group level clusters can potentially be used to aid clinical decision making and recover patterns in the data that to date may otherwise have gone undetected. In future work, we will further refine and apply the tool to gain valuable clinical insights such as better understanding/prediction of bDMARD and other treatment effects and stimulate new research questions in ways that advance our current approach to the disease.
REFERENCES: [1] P. Machado, R. Landewé, C. Tuyl, M. B. Hermann-Hansen, J. C. Gossert, and D. van der Heijde, “Cluster analysis in early axial spondyloarthritis predicts poor outcome in the presence of peripheral articular manifestations,” Annals of the Rheumatic Diseases , vol. 74, no. 12, pp. 2191-2199, 2021.
[2] S. Lloyd, “Least squares quantization in PCM,” IEEE Transactions on Information Theory , vol. 28, no. 2, pp. 129-137, March 1982.
[3] J. MacQueen, “Some methods for classification and analysis of multivariate observations,” in Proceedings of the Fifth Berkeley Symposium on Mathematical Statistics and Probability , vol. 1, pp. 281-297, 1967.
Acknowledgments: NIL.
Disclosure of Interests: Daniel Burrows: None declared, Matthias Ehrhardt: None declared, Rosemarie Barnett Rosemarie Barnett has received an axSpA research grant from UCB, and a one-off payment from Pfizer for developing axSpA educational content for HCPs., Rosemarie Barnett has received an axSpA research grant from UCB, and a one-off payment from Pfizer for developing axSpA educational content for HCPs., Raj Sengupta Raj Sengupta has previously held unrelated grants from Abbvie, Novartis, Pfizer and UCB and received honoraria for giving talks from Abbvie, Alfasigma, Pfizer, Novartis and UCB. RS has represented Abbvie and Novartis at NICE technology appraisals., Raj Sengupta has previously held unrelated grants from Abbvie, Novartis, Pfizer and UCB and received honoraria for giving talks from Abbvie, Alfasigma, Pfizer, Novartis and UCB. RS has represented Abbvie and Novartis at NICE technology appraisals.