fetching data ... 
Background: Systemic Lupus Erythematosus (SLE) is a chronic multisystem autoimmune disorder that is a result of a complex interplay of genetic, environmental, and immunological factors. Recent research has shown growing evidence linking gut dysbiosis to SLE pathogenesis. Alterations in gut microbial composition—particularly a reduced alpha(α) and beta(β) diversities have emerged as key modulators of disease activity. However, studies on gut dysbiosis in SLE patients are limited from this part of the world. This study was designed to investigate dysbiosis in SLE with focus on its change with treatment.
Objectives: To estimate the alpha, beta diversity and dysbiosis index of gut microbes in patients with SLE, compared with patients with rheumatoid arthritis (RA) as autoimmune disease control and healthy controls (HC).
To investigate the diversities of gut microbes in patients with SLE, and to correlate with disease activity.
Methods: This was a cross-sectional, observational, single-centre study involving 52 SLE patients meeting the 2019 ACR/EULAR classification criteria, along with 16 RA patients (ACR/EULAR, 2010) and 32 age-matched healthy controls The study was approved by Institutional Ethics Committee (IEC 1418/16.08.23). Clinical data including SLEDAI and treatment details were recorded in a predesigned proforma. Fecal DNA was isolated using the Translational Health Science and Technology Institute (THSTI) manual method. The full-length 16S rRNA gene (V1–V9 regions) was amplified using 27f/1492r primers. Polymerase Chain Reaction (PCR) was performed in a 50µl reaction volume using 1ng template DNA, 5pmol primers concentration and NEB Q5® High-Fidelity 2X Master Mix. PCR products (~1.6 kb) were confirmed on agarose gel, purified, quantified, and sequenced using the Oxford Nanopore MinION platform after library preparation with native barcoding kits. For bioinformatics, raw Nanopore reads were base-called, quality-checked (Fast QC), and filtered (NanoFilt). Taxonomic classification was done using Kraken2, and downstream analysis was conducted in R using packages such as phyloseq , microbiome , vegan , and DESeq2 . Differentially abundant taxa (163 OTUs) were identified (p <0.05) and used for compositional and statistical analyses. Alpha diversity (Shannon, Simpson, Observed) and beta diversity (PCoA using weighted UniFrac) were analyzed, and compared using Wilcoxon test and PERMANOVA. A dysbiosis index was calculated using Bray-Curtis distances and Euclidean distances from HC centroid in PCoA space. Compositional differences at various taxonomic levels were assessed, and LEfSe analysis (LDA >2.0, p <0.05) identified significantly enriched taxa. Species-level correlations with disease severity were explored using Spearman’s correlation and visualized via heatmaps.
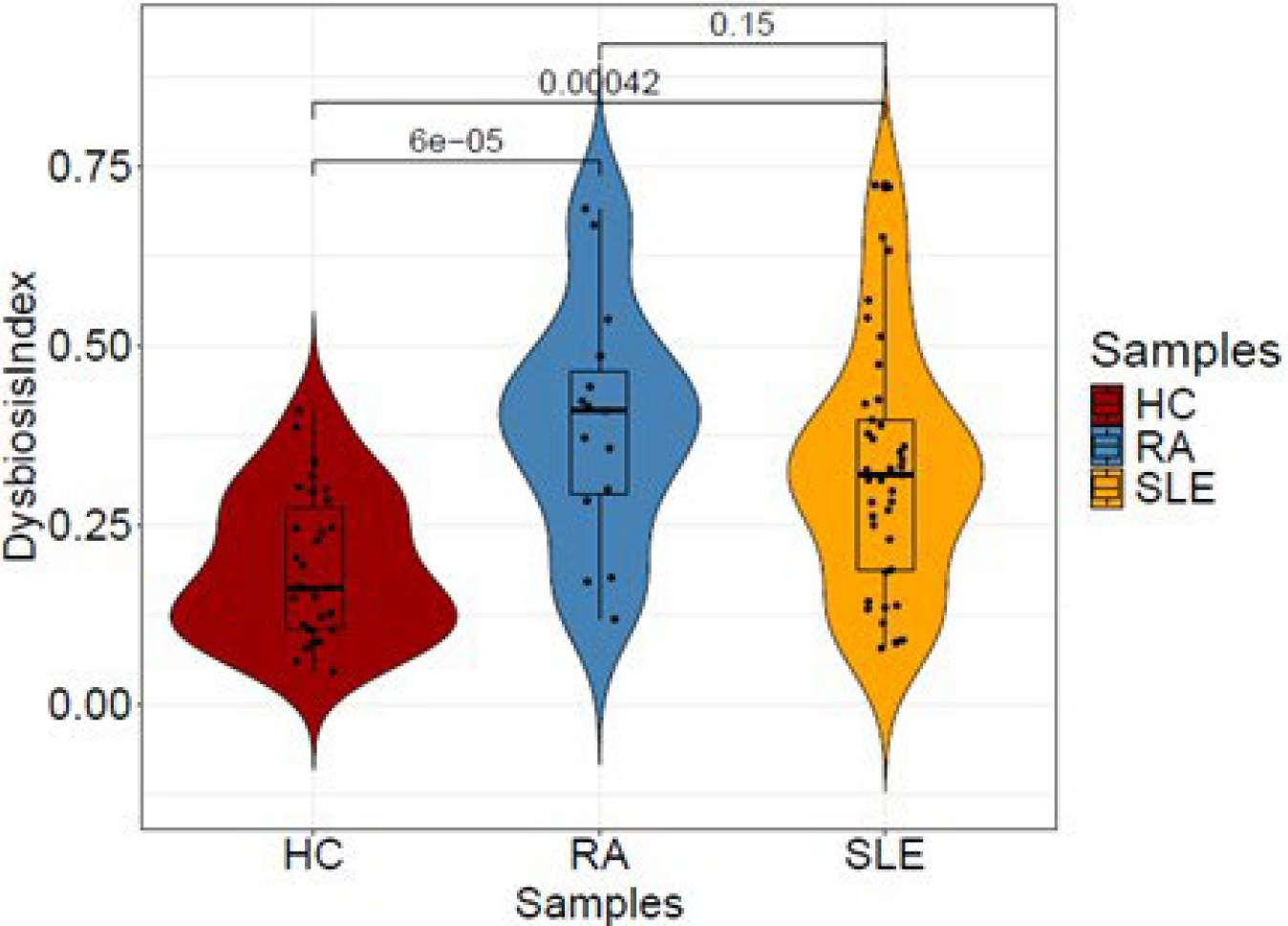
Results: Among the SLE patients enrolled, the most common manifestations were mucocutaneous involvement (86.5%) followed by arthritis (61%) and nephritis (59%) respectively. Majority of patients (64%) had moderate to severe disease activity (SLEDAI 2K ≥7). Alpha and beta diversity analyses revealed reduced microbial richness and community dispersion in SLE and RA, suggesting disrupted microbial homeostasis. Higher dysbiosis index was obtained in both SLE and RA groups compared to the HC group (p <0.001; Figure 1). Gut dysbiosis was observed in SLE and RA patients, marked by reduced Bacillota and increased Pseudomonadota at the level of phylum compared with healthy controls. Patients with RA showed a higher abundance of Pseudomonadota than those with SLE. A distinct microbial signature with elevated levels of pro-inflammatory bacteria such as Streptococcus mutans , Phocaeicola vulgatus , and Enterococcus fecalis was observed in patients with SLE. Disease activity (SLEDAI-2K) correlated with microbial profiles, where mild cases showed higher levels of A. muciniphila and S. mutans , while severe cases were marked by increased P. vulgatus and E. fecalis , suggesting a progressive dysbiosis linked with disease severity.
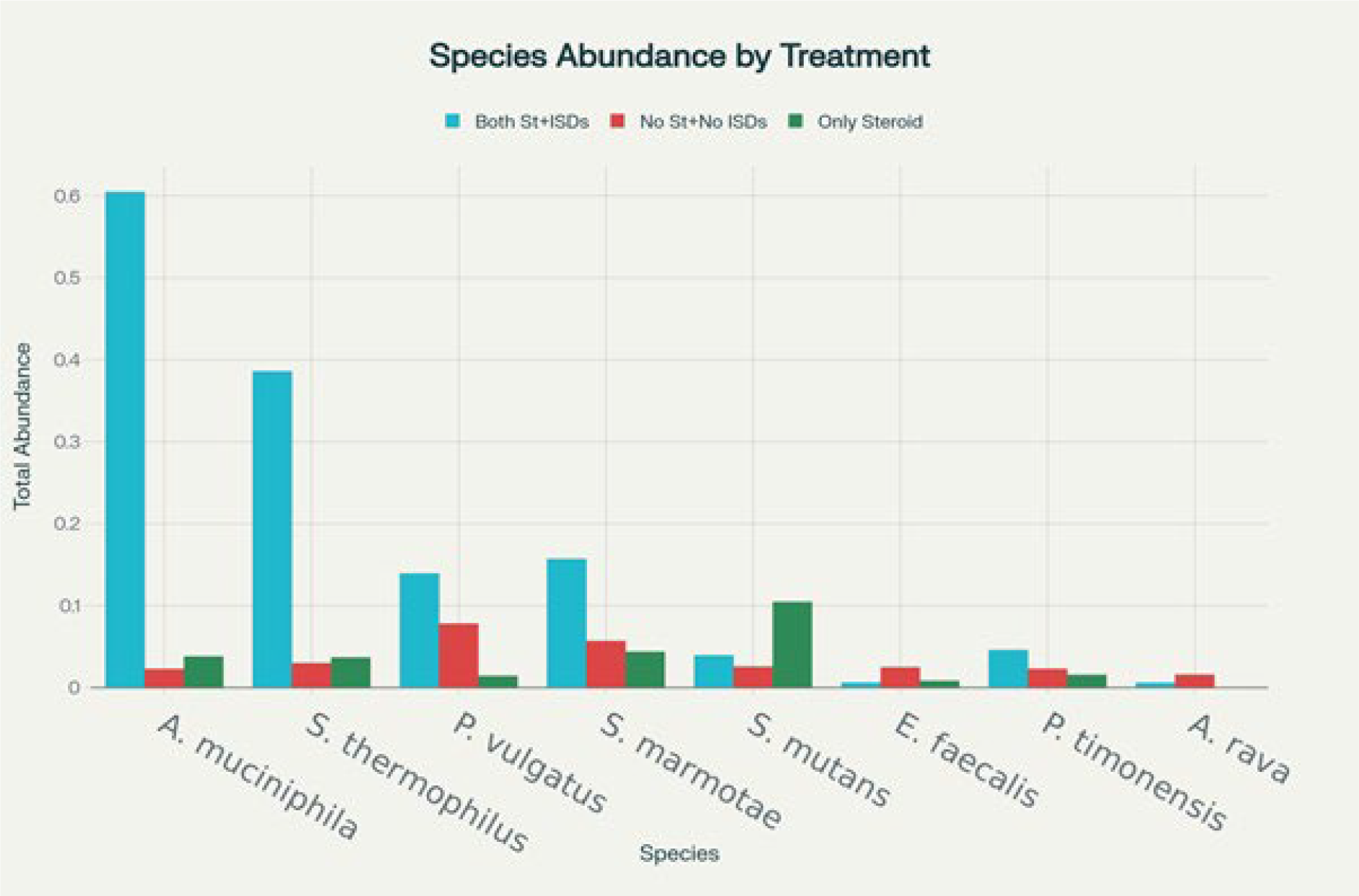
When SLE patients were categorised as per the treatment received at time of sampling, interesting results were observed. Patients who received both steroids and immunosuppressive drugs had abundance of A. muciniphila, S. thermophilus, Blautia, Ligilactobacillus which are known to promote gut barrier functions through gut mucus building, tight junction repair and promote a metabolic shift towards anti-inflammatory metabolites. Whereas patients who were treatment naïve had more of pathogenic bacteria like C. Koseri, D. succinatiphilus, P. vulgatus, E. faecalis, P. timonensis , & A. rava which are associated with leaky gut (Figure 2).These results point towards restoration of microbiota with treatment in SLE patients.
Conclusions: There is increased gut dysbiosis in SLE, showing enrichment of potential pro-inflammatory or opportunistic bacteria. SLE microbiota may reflect increased mucosal barrier disruption and systemic immune activation but treatment with immunosuppressive drugs provide restoration and maintenance of symbiotic propensity. Longitudinal mechanistic studies and metabolomics may establish causal relationships and provide microbiome-based biomarkers for therapeutic targets.
Violin plot showing dysbiosis index of HC, RA, and SLE groups
Microbiota species abundance among various treatment groups in SLE patients
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.