fetching data ... 
Background: Hydroxychloroquine (HCQ) was originally synthesized as the antimalarial drug. However, it is now primarily used as the immunomodulatory drug and is recommended for all the patients with systemic lupus erythematosus (SLE) unless contraindicated [1, 2]. HCQ reduces the flare risk in the clinical quiescent (CQ) patients with SLE, and recent report also reveals that HCQ contributes to the withdrawal of low-dose glucocorticoid [3]. Whereas potential mechanisms of action of the HCQ are thought to be inhibition of antigen presentation and Toll-like receptor signaling [1], its effect on immune cell subsets in the patients with SLE in CQ state remains elusive.
Objectives: To evaluate the effect of hydroxychloroquine (HCQ) on the immune system in patients with systemic lupus erythematosus (SLE) without clinical activity.
Methods: Peripheral blood samples from patients with SLE who received remission-induction therapy and have achieved clinically quiescent (CQ) state, defined as clinical SLE disease activity (cSLEDAI) score of 0 for more than 6 months, were collected. We comprehensively analyzed the changes of immune cells in the peripheral blood before induction therapy and after achieving the CQ state by flow cytometry and compared those among patients with or without the use of HCQ.
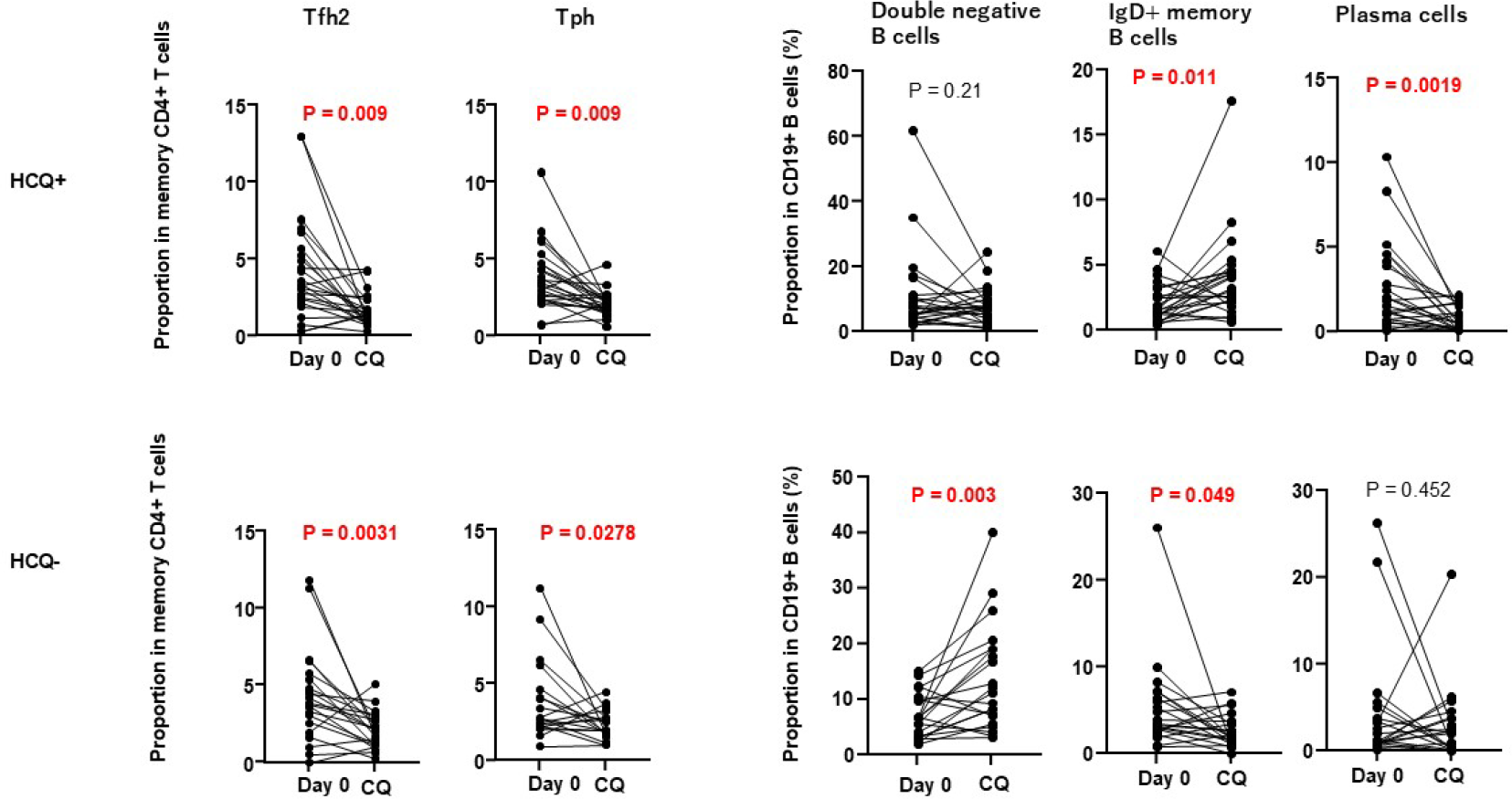
Results: We enrolled 45 patients with SLE in the analyses. The mean age was 45, and 39 (86.7%) were female. The mean SLEDAI at baseline was 16.7±9.4. The mean initial dose of prednisolone (PSL) was 48±14 mg/day, and most of the patients were treated with cyclophosphamide or mycophenolate mofetil. At the CQ state, the mean dose of PSL was 3.3±2.3 mg/day, and 24 (53.3 %) received HCQ. The concomitant immunosuppressive drugs and clinical features at baseline were comparable between the HCQ and non-HCQ groups. The proportions of Tfh2 and total Tph among memory CD4+ T cells decreased from baseline regardless of HCQ use. In contrast, the reduced proportion and the total number of plasma cells among B cells were only observed in the HCQ group (P < 0.01 and P =0.048, respectively). The proportions of IgD+ memory B cells among B cells increased in the HCQ group whereas decreased in the non-HCQ group (P = 0.01, P= 0.048, respectively). The proportion of IgD-CD27- B cells increased and that of transitional B cells decreased only in the non-HCQ group (P < 0.01 and P = 0.029, respectively). Myeloid subsets such as dendritic cells, monocytes and neutrophils all increased in the HCQ group although similar trends were also observed in the non-HCQ group, which indicated that the increase of the myeloid subsets from baseline was observed in the CQ state of SLE regardless of HCQ use. Taken together, HCQ may affect the differentiation of B cells subsets into plasma cells and IgD-CD27- cells in CQ state of SLE.
Conclusions: The use of HCQ in CQ sate of patients with SLE affect the B cell subsets rather than those of T cells and may modulate the disease.
REFERENCES: [1] Schrezenmeier E, Dörner T. Mechanisms of action of hydroxychloroquine and chloroquine: implications for rheumatology. Nat Rev Rheumatol 2020;16(3):155-66.
[2] Fanouriakis A, Kostopoulou M, Andersen J, Aringer M, Arnaud L, Bae SC, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Dis 2024;83(1):15-29.
[3] Katsumata Y, Inoue E, Harigai M, Cho J, Louthrenoo W, Hoi A, et al. Risk of flare and damage accrual after tapering glucocorticoids in modified serologically active clinically quiescent patients with systemic lupus erythematosus: a multinational observational cohort study. Ann Rheum Dis 2024;83(8):998-1005.
Acknowledgments: NIL.
Disclosure of Interests: None declared.