fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a heterogeneous, multisystem autoimmune disease characterized by dysregulated innate and adaptive immune responses. Prominent among these is activation of the type I interferon (IFN) pathway, reflected by increased expression of interferon-stimulated genes (ISGs).
Objectives: To quantify a 28-gene type I interferon–stimulated gene (ISG) score in SLE patients and healthy controls, and to evaluate its association with disease activity, serologic markers, and DNASE1L3 mutation status.
Methods: Peripheral blood samples were obtained from SLE patients and healthy controls. Total RNA was extracted using the QIAamp RNA Blood Mini Kit. Expression of 28 ISGs was quantified and normalized to housekeeping genes. An ISG score was calculated using a previously described z-score–based approach [1]. For each gene, expression values were standardized relative to healthy controls using a robust z-score formula based on the median and median absolute deviation (MAD): robust z ij = (X ij − median j )/ (MAD j × 1.4826 ) where X ij represents the expression of gene j in sample i . The overall ISG score for each sample was obtained by summing standardized expression values across all 28 genes. Associations between ISG score, serologic markers and disease activity (via the SLE disease activity index “SLEDAI”, where patients were considered “inactive-mild” if they had a score 0-4, and “moderate-severe” if they had a score of ≥ 6 points) were assessed using non-parametric statistical methods.
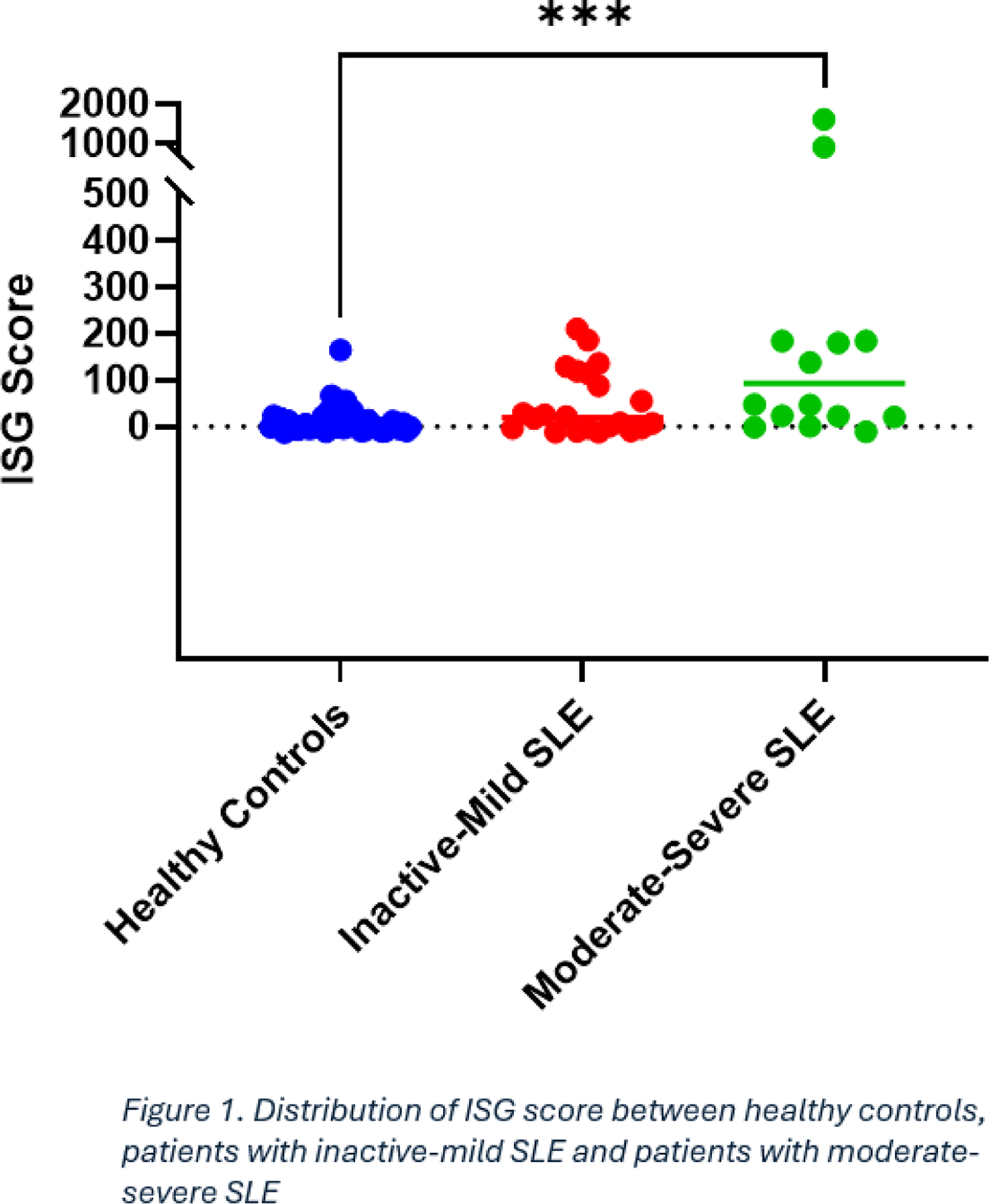
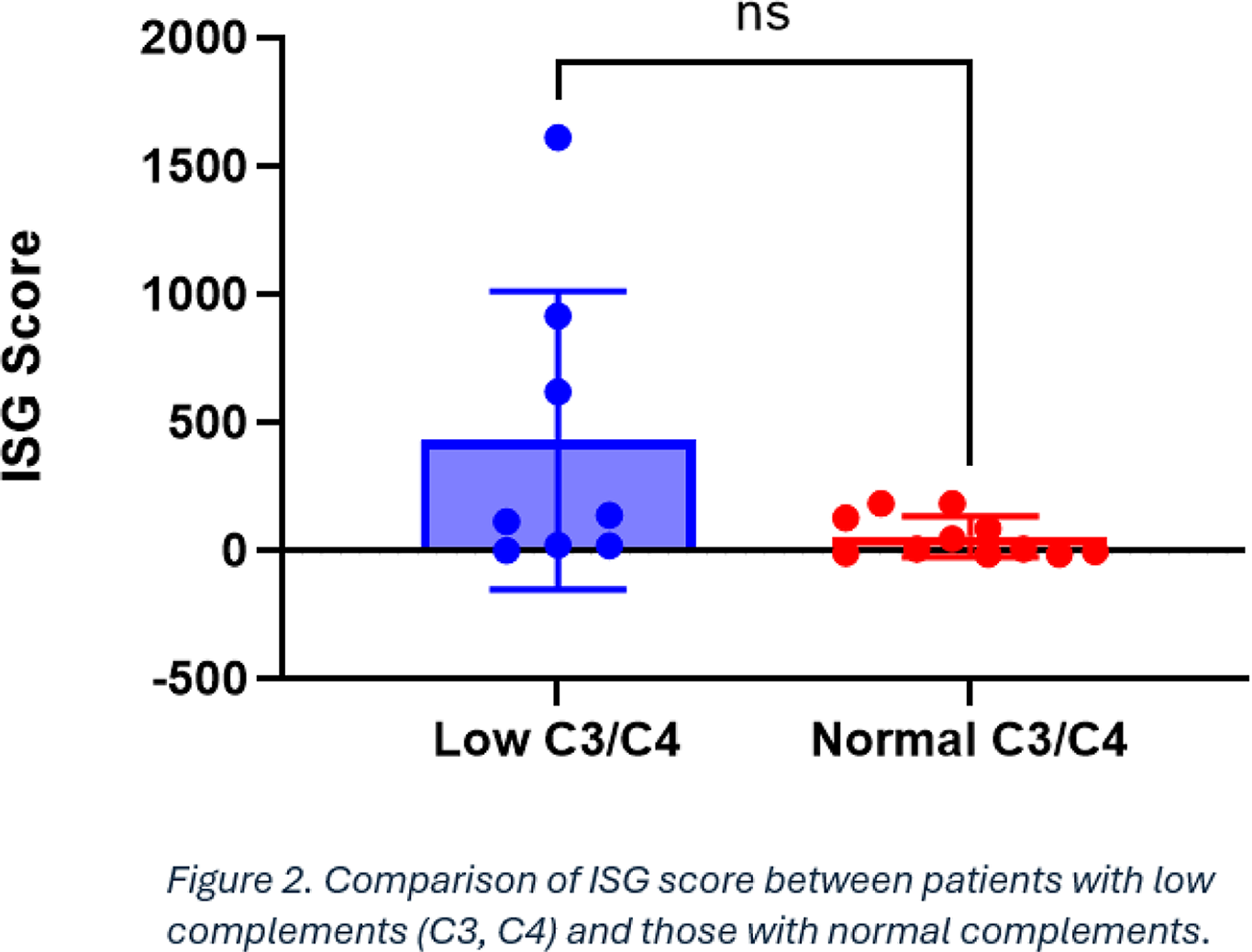
Results: A total of 70 subjects were included in this study. Of these, there were 20 SLE patients (of which 5 patients with known DNASE1L3 mutations) and 50 healthy controls. SLE patients with inactive-mild disease had a slightly higher ISG score compared to healthy controls (median = 26.42 vs 2.2, p = 0.3826) but not to a statistically significant level. Patients with moderate-severe SLE had a significantly higher ISG score compared to healthy controls (median=24 vs 2.2, p = 0.0006). However, SLE patients in the two groups had largely overlapping ISG scores despite varying clinical disease activity (Figure 1). Additionally, there was only a moderate association between ISG scores and SLEDAI scores (Spearman ρ = 0.49, p = 0.003). With regards to serologic markers, the ISG score was strongly correlated with anti-dsDNA antibody levels but only in patients with SLE without DNASE1L3 mutations (Spearman ρ = 0.69, p = 0.005). There was no significant correlation between ISG score complement levels (C3, C4 and C1q) but patients with low C3 and C4 tended to have a higher ISG score (Figure 2, p = 0.007).
Conclusions: Type I interferon pathway activation, as measured by a 28-gene ISG score, is variably associated with clinical disease activity supporting its role as a biologic endotype marker rather than a direct measure of disease severity. Distinct relationships between ISG expression and serologic markers in DNASE1L3-deficient versus non-deficient patients highlight underlying immunogenetic heterogeneity within SLE. Further observations longitudinally and with consideration of medication effects are needed to better understand and better utilize the ISG score in SLE care.
REFERENCES: [1] Feng X, Wu H, Grossman JM, Hanvivadhanakul P, FitzGerald JD, Park GS, Dong X, Chen W, Kim MH, Weng HH, Furst DE, Gorn A, McMahon M, Taylor M, Brahn E, Hahn BH, Tsao BP. Association of increased interferon-inducible gene expression with disease activity and lupus nephritis in patients with systemic lupus erythematosus. Arthritis Rheum. 2006 Sep;54(9):2951-62. doi: 10.1002/art.22044. PMID: 16947629.
Acknowledgments: NIL.
Disclosure of Interests: None declared.