fetching data ... 
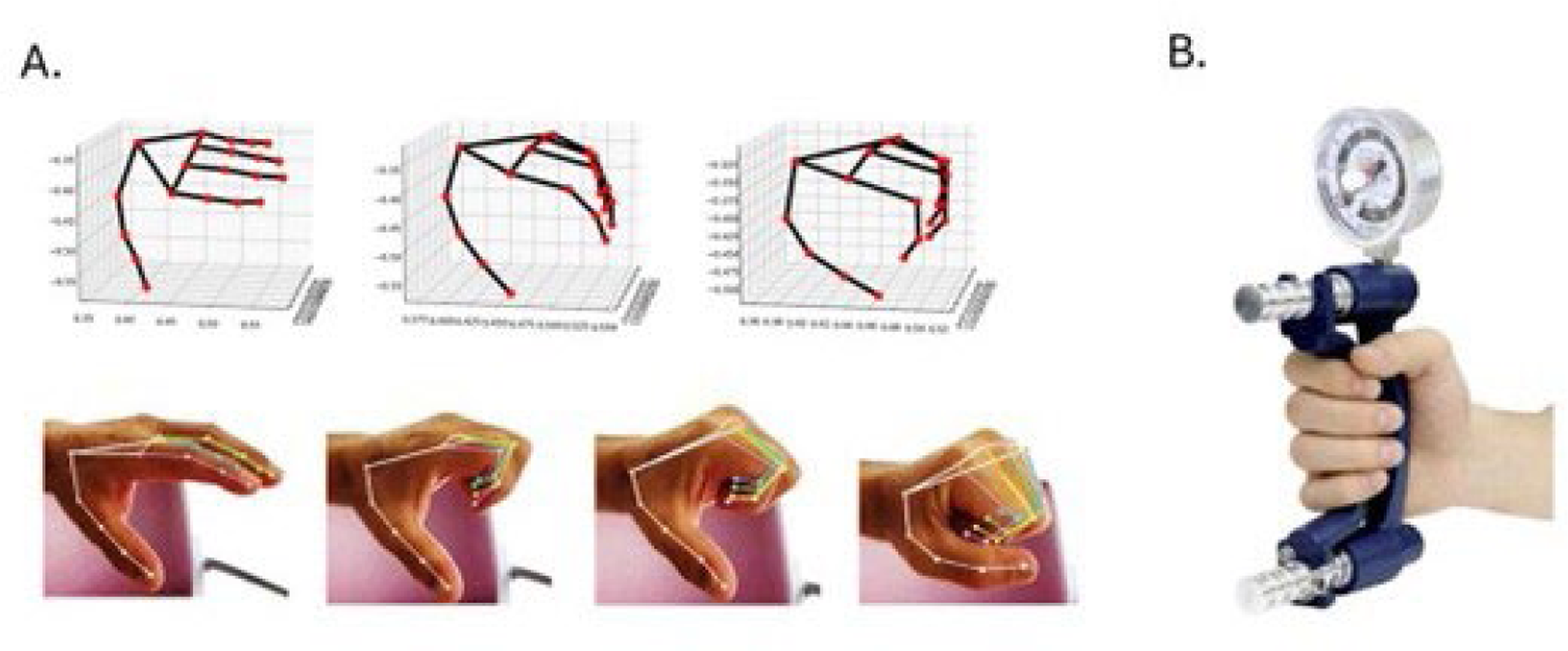
Background: Automated single-camera motion capture of joint movement has emerged as a promising digital biomarker in inflammatory arthritis. We previously demonstrated that repeated fist closure recorded by a smartphone camera (MeFISTO prompt) (Figure 1) allows extraction of kinematic features of hand joints that correlate with disease activity in patients with rheumatoid arthritis (RA). For application in remote patient monitoring, further clinical validation is required, particularly with respect to functional outcomes.
Objectives: To evaluate whether smartphone-derived kinematic measures of metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints can infer grip strength.
Methods: We prospectively included 102 patients with inflammatory arthritis (RA, spondylarthritis, crystal arthropathy and systemic sclerosis) with 1–6 study visits at the Lausanne University Hospital (CHUV). During each visit, hand motion was recorded while patients performed five rapid iterations of fist closures (MeFISTO) using smartphone cameras. A total of 223 analyzable hand videos were obtained. Video data were processed using the MediaPipe Pippi package (version 0.10.10) to identify hand landmarks. Joint angles were calculated frame by frame using the normalized dot product of joint vectors. Ten kinematic metrics were extracted, including range of motion, mean absolute angular velocity and acceleration, and their respective maxima at MCP and PIP joints. Grip strength was measured using a handheld hydraulic hand dynamometer. Clinical variables included the Disease Activity Score in 28 joints (DAS28) and the physician global assessment.
Spearman’s rank correlation was applied to assess associations involving non-normally distributed variables. Correlation strength was categorized as follows: Spearman’s ρ values from 0.00 to ±0.30 were considered weak, values from ±0.40 to ±0.60 moderate, and values from ±0.60 to ±0.90 strong. Statistical significance was set at a two-sided p value < 0.05, with corresponding 95% confidence intervals.
Results: Among 102 patients aged 40–92 years, 71 were female (69,6%). Diagnoses comprised 84 (82,4%) rheumatoid arthritis, 13 (11,8%) spondylarthritis, 2 (2,0%) systemic sclerosis, and 2 (2,0%) microcrystalline arthritis. At least moderate disease activity (DAS28 ≥ 3.2) was observed in 23 patients (22,6%). Regarding follow-up, 53 patients (52%) attended a single visit, 34 (32,3%) had 1–3 visits, and 15 (14,7%) had more than 3 visits. Lower disease activity was at least moderately (maximum correlation ρ = -0.302) associated with higher mean MCP velocity and acceleration and higher mean PIP velocity and acceleration in right hands (N = 33; all p ≤ 0.006), left hands (N = 102; all p ≤ 0.002), and the combined sample (N = 135; all p < 0.001), with the strongest association for MCP maximum velocity in right hands (ρ = -0.722). Higher grip strength correlated significantly with higher MCP mean velocity and both MCP and PIP mean acceleration in both hands (N = 64; ρ from 0.367 to 0.500; all p < 0.003). Larger range of motion was significantly associated with less sever disease activity on both hands (N=134; all p=0.004; max ρ = -0.30). Higher grip strength was associated with lower disease activity (N = 55; ρ = −0.308; p = 0.022) (Table 1.)
Conclusions: Smartphone-based, AI-derived kinematic measures of hand motion correlate with both disease activity and grip strength, supporting their potential role as digital biomarkers of disease activity and functional impairment in inflammatory arthritis.
A. MeFISTO vectors, B. Hydraulic hand dynanometer.
Spearman’s correlations between video-derived measurements and disease activity, and between video-derived measurements and grip strength
| Hand side | Disease activity (DAS28) correlation | Grip strength (kgs) correlation | |||||
|---|---|---|---|---|---|---|---|
| Spearman’s | Significance | N | Spearman’s | Significance | N | ||
| Delta flexion MCP (°) | Left | -0,30 | 0,002 | 102 | -0,03 | 0,822 | 46 |
| Right | -0,59 | <,001 | 32 | 0,06 | 0,807 | 18 | |
| Delta flexion PIP (°) | Left | -0,39 | <,001 | 102 | -0,14 | 0,339 | 46 |
| Right | -0,49 | 0,004 | 33 | 0,12 | 0,632 | 18 | |
| Mean absolute angular velocity MCP | Left | -0,42 | <,001 | 102 | 0,54 | <,001 | 46 |
| Right | -0,54 | 0,001 | 32 | 0,56 | 0,017 | 18 | |
| Mean absolute angular velocity PIP | Left | -0,44 | <,001 | 102 | 0,35 | 0,016 | 46 |
| Right | -0,60 | <,001 | 33 | 0,45 | 0,063 | 18 | |
| Mean absolute angular acceleration MCP | Left | -0,44 | <,001 | 102 | 0,46 | 0,001 | 46 |
| Right | -0,59 | <,001 | 33 | 0,51 | 0,031 | 18 | |
| Mean absolute angular acceleration at the PIP | Left | -0,45 | <,001 | 102 | 0,38 | 0,009 | 46 |
| Right | -0,60 | <,001 | 33 | 0,47 | 0,047 | 18 | |
| Max. absolute angular velocity at the MCP | Left | -0,32 | 0,001 | 102 | 0,05 | 0,753 | 46 |
| Right | -0,72 | <,001 | 33 | 0,27 | 0,278 | 18 | |
| Max. absolute angular velocity at the PIP | Left | -0,40 | <,001 | 102 | 0,13 | 0,395 | 46 |
| Right | -0,47 | 0,006 | 33 | 0,32 | 0,203 | 18 | |
| Max. absolute angular acceleration at the MCP | Left | -0,34 | 0,001 | 102 | 0,12 | 0,425 | 46 |
| Right | -0,69 | <,001 | 33 | 0,33 | 0,176 | 18 | |
| Max. absolute angular acceleration at the MCP | Left | -0,43 | <,001 | 102 | 0,20 | 0,192 | 46 |
| Right | -0,58 | <,001 | 33 | 0,45 | 0,058 | 18 | |
REFERENCES: [1] Venerito V, Manigold T, Capodiferro M, Markham D, Blanchard M, Iannone F, Hügle T. Single-camera motion capture of finger joint mobility as a digital biomarker for disease activity in rheumatoid arthritis. Rheumatol Adv Pract. 2025;9(2):rkae143. doi:10.1093/rap/rkae143.
Acknowledgments: NIL.
Disclosure of Interests: Léna Ghika: None declared, Cinja Nadana Koller: None declared, Jules Maglione: None declared, Vincenzo Venerito Abbvie Boehringer Ingelheim Galapagos – AlfaSigma GSK Janssen Lilly Novartis Pfizer UCB Werfen, Tobias Manigold: None declared, Deborah Markham: None declared, Thomas Hügle Abbvie, GSK, J&J, UCB, Atreon SA.