fetching data ... 
Background: Patients with vasculitis are often suitable for remote management via electronic forms once their condition is in remission or has low disease activity. However, identifying the subgroup of patients at risk for disease flares is crucial. Remote management provides patients with convenient technology and supports the principle of delivering the right care to the right patient. To ensure patient safety, remote assessments must accurately reflect disease activity.
Objectives: We aimed to assess remote management for identifying active vasculitis by comparing patient questionnaires with clinician assessments, and to compare these results between giant cell arteritis (GCA) and ANCA-Associated Vasculitis (AAV) patients.
Methods: We have employed a remote management system using Microsoft Forms and Rhadio to review patients [1]. Questionnaires are sent to patients on our waiting list, and their responses are reviewed to assess disease activity. If a flare is suspected, the patient is contacted for an appointment to adjust treatment. This process has been instrumental in managing the patient backlog accrued due to the COVID-19 pandemic [2,3]. The remote assessment questionnaire includes self-reported Birmingham Vasculitis Assessment Score (BVAS) and the ANCA-Associated Vasculitis Patient-Reported Outcome (AAVPRO). This information is reviewed by a clinician who will determine if, when and in what format patients require further appointments. We analysed vasculitis remote consultation data from Rhadio between 2022-2025. Repeat patient forms were included. Patients were classified as ´stable´or ´unstable´ based on self-reported BVAS scores, with a focus on those who had a visit within three months of completing the questionnaire. Patients were further stratified by patient-reported control of the condition (good vs poor), and we evaluated their distribution according to remote disease activity assessment by clinician. The analysis was conducted on the entire cohort and separately on AAV and GCA subgroups. We used Chi-square and Wilcoxon rank-sum tests to compare variables, with statistical significance set at p<0.05. All analyses were performed using SAS (Version 9.4).
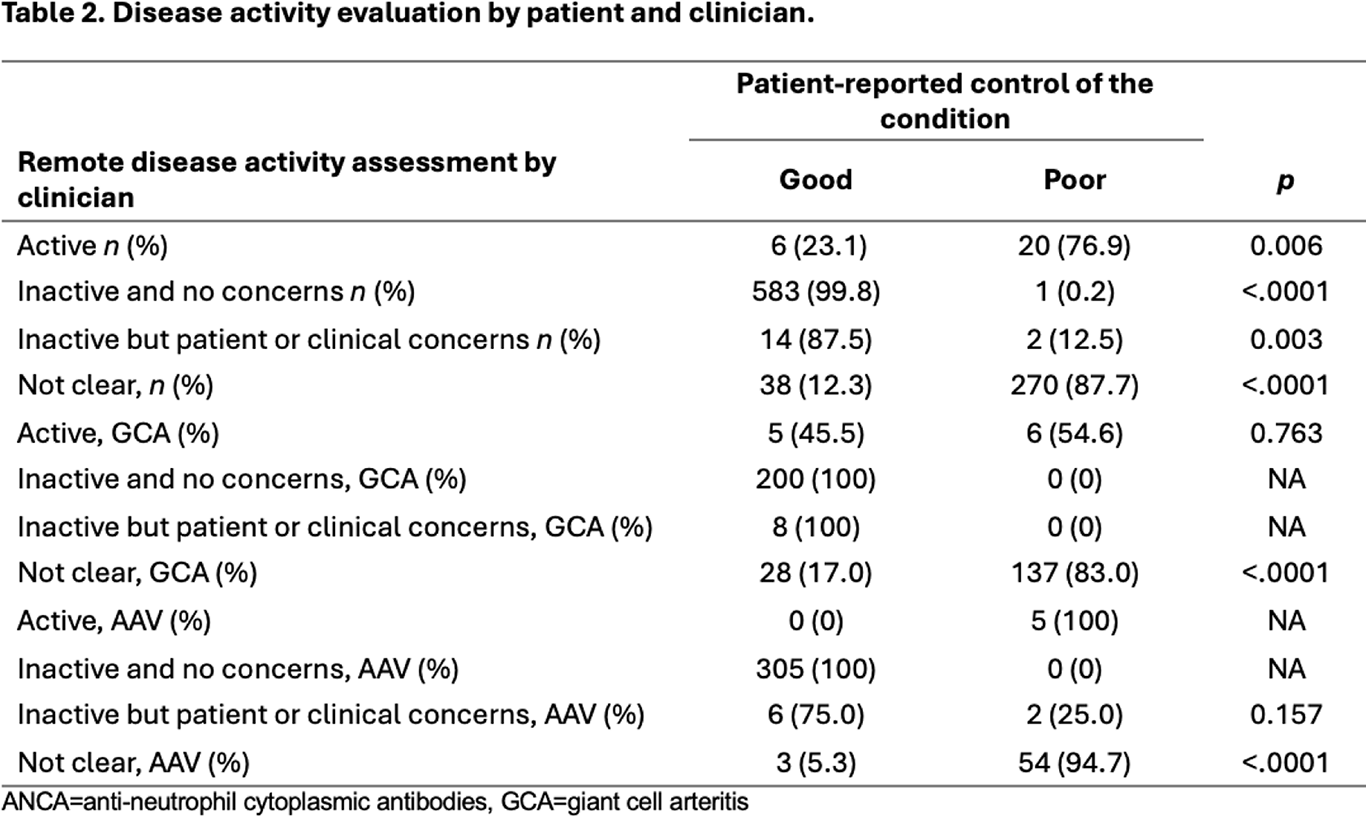
Results: A total of 759 assessments in a cohort of 268 patients (99 with GCA and 169 with AAV) were included in the study. Significantly higher BVAS and AAVPRO scores were observed in the unstable vasculitis group (p <.0001) (Table 1). The vasculitis cohort demonstrated a disease state of stable in 53.4 % of patients and unstable in 46.6 %. Analysis of the primary subgroups revealed a similar pattern, with 58.5% of AAV patients and 55.0% of GCA patients classified as stable. Patients in the unstable vasculitis cohort and its subgroups (AAV and GCA) required more appointments within 90 days of questionnaire completion (p <.0001, p = 0.0007, and p = 0.0006, respectively). Patient and clinician assessments aligned for inactive disease in all groups (vasculitis, GCA, and AAV). With active disease, agreement was found in the overall vasculitis and AAV groups (Table 2).
Conclusions: Remote clinical management is a reliable method in predicting stable and active disease in vasculitis patients. Limitations include the lack of formal validation for the AAVPRO in GCA patients and for the self-reported BVAS, which affects the generalizability of the results. In conclusion, the clinician’s remote assessment aligns with patient self-reporting, supporting its reliability for patient-cantered care.

REFERENCES: [1] Soni, A. et al. (2022). P115 Remote clinical management: incorporating electronic assessment of patients with rheumatic diseases into standard clinical pathways and comparison to in-person assessment. Rheumatology, 61(Supplement_1), keac133-114.
[2] Malley, T. et. al. “POS0152-HPR REMOTE CLINICAL MANAGEMENT: INCORPORATING ELECTRONIC ASSESSMENT OF PATIENTS WITH RHEUMATICDISEASES INTO STANDARD CLINICAL PATHWAYS DURING THE COVID-19 PANDEMIC: A PILOT STUDY.” (2021):289-290.
[3] Kurzeja, D. et al (2023). P005 Using novel remote electronic monitoring to measure and manage the Rheumatology Clinic backlog generated by COVID-19, Rheumatology, Volume 62, Issue Supplement_2, April 202.
Acknowledgments: NIL.
Disclosure of Interests: None declared.