fetching data ... 
Background: Opioids are frequently prescribed for pain-management in patients with rheumatic and musculoskeletal conditions (RMDs). However, they are associated with several adverse events (AEs), including serious AEs such as delirium, fractures, dependence, premature mortality and those that are common but important to patients, such as constipation. Currently, there are no available tools that estimate patients’ personalised risk of several opioid-related AEs at the point of treatment initiation. Existing clinical prediction models (CPMs) typically focus on predicting one AE at a time, which may lead to an inaccurate estimation of patients’ risk of experiencing multiple AEs. More advanced multi-outcome modelling approaches are therefore needed to directly predict combinations of AEs and better identify high-risk patients.
Objectives: The overall aim is to evaluate if CPMs designed for multi-outcome prediction outperform traditional methods for single-outcome CPM methods to predict AEs associated with pain medications prescribed for RMDs, such as opioids.
The specific objective is to develop, internally and externally cross-validate, and compare CPMs for eight possible combinations of constipation, delirium, and fractures in patients with RMDs.
Methods: We used data from Clinical Practice Research Datalink Aurum linked with Hospital Episode Statistics from January 2006 to October 2021. Eligible participants were UK adults diagnosed with an RMDs who initiated opioid treatment during this period, with no cancer diagnosis or cancer-related opioid prescription in the preceding five years. The follow-up period was one year from opioid initiation.
Eight CPMs were developed and validated, including three single-outcome logistic regression models, a univariate combined model, in which risks from the three LR models were combined, alongside a multinomial logistic regression (MLR) model, a multivariate Bayesian probit (MTBP) model, a probabilistic classifier chain (PCC) model, and a multi-target classification tree (MTCT) model.
Missing data were handled using single regression imputation, and predictors were selected using clinical expertise and the Least Absolute Shrinkage and Selection Operator method. Models were validated using internal-external cross-validation (IECV) across nine UK regions. Model performance was assessed for the predicted risk of individual AEs and predicted risk of AE combinations, using discrimination (Area Under the Curve [AUC] for individual AEs and the polytomous discrimination index [PDI] for AE combinations) and calibration (intercept and slope).
Results: The cohort included 1,407,570 patients (median age 60 years; 59.6% females). Across IECV, all models demonstrated an almost identical performance when predicting individual AEs. Calibration slopes ranged from 0.98 to 1.01, and calibration intercepts from −0.02 to 0.00 across outcomes, indicating near-perfect calibration. Discrimination was also comparable across models, with AUC = 0.70 for constipation, 0.89 (95% CI 0.88–0.90) for delirium, and 0.73–0.74 for fractures
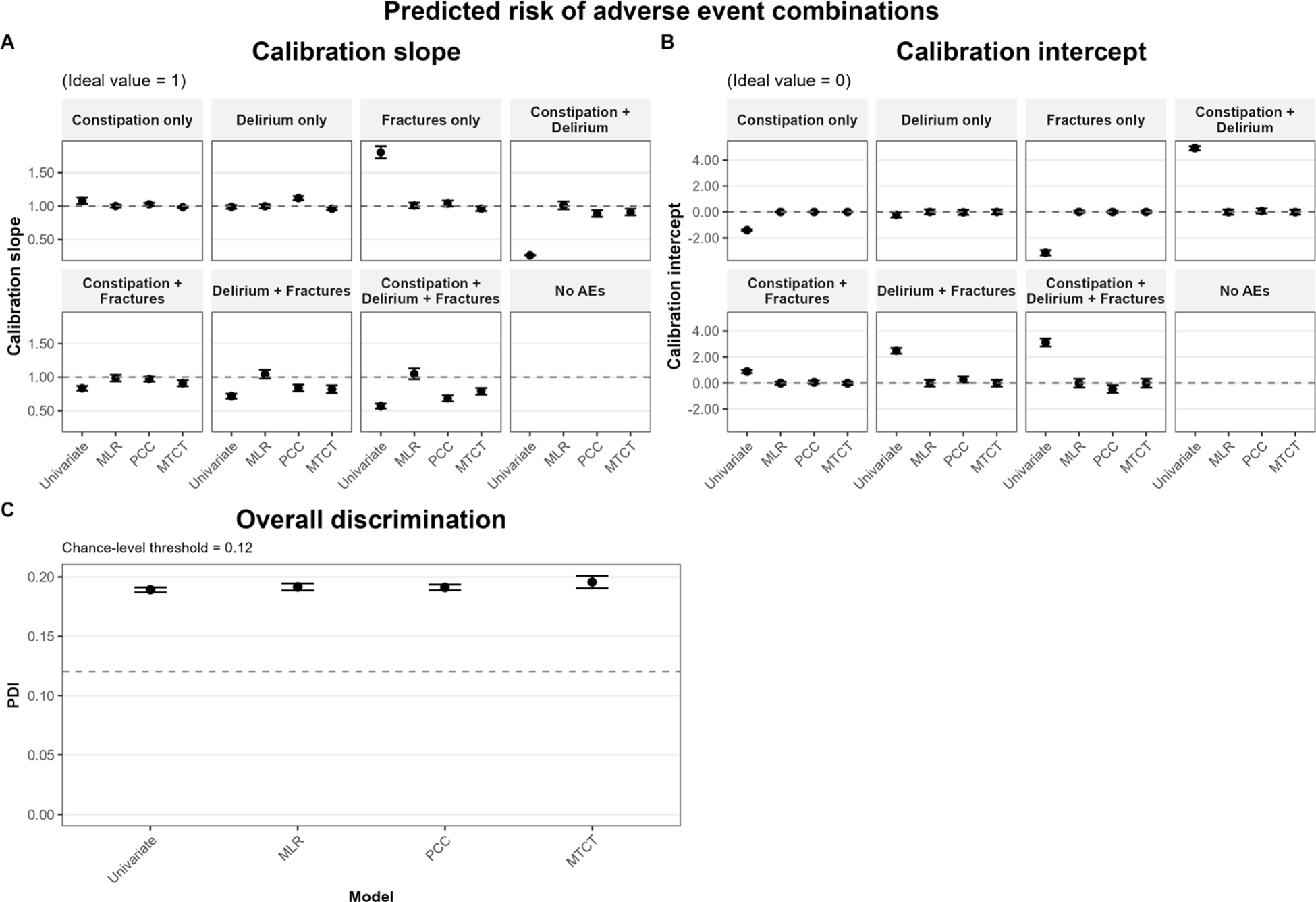
In contrast, differences emerged when predicting combinations of AEs. The univariate combined model showed substantial miscalibration across outcome combinations, with calibration slopes ranging from 0.27 to 1.80 and intercepts from −3.15 to 4.91, indicating both over- and under-prediction of absolute risk. In comparison, the MLR model demonstrated calibration slopes consistently close to 1 (0.98–1.05) and intercepts close to 0 across all eight outcome combinations (-0.02- 0.00) (Figure 1). Other multi-outcome models showed intermediate performance (Figure 1). PCC had calibration slopes ranging from approximately 0.84 to 1.12 across outcome categories, while MTCT showed slopes ranging from approximately 0.79 to 0.98. Calibration intercepts for PCC and MTCT generally remained close to zero across categories (approximately −0.04 to 0.26 for PCC and −0.02 to 0.00 for MTCT). Discrimination for AE combinations was moderate and similar across models, with overall PDI values of 0.19–0.20, exceeding the chance-level threshold of 0.12 (Figure 1).
Conclusions: To better support prescribing decisions, CPMs specifically designed to predict combinations of AEs provided more reliable estimates of patients’ risk of experiencing multiple opioid-related AEs than approaches based on combining single-outcome predictions. Importantly, this improved estimation of combined risk was achieved without compromising the accuracy of predictions for individual AEs. Among the evaluated methods, MLR showed the most stable performance across outcome combinations and regions. These findings highlight the potential of multi-outcome CPMs for medications prescribed for RMDs associated with multiple harms when combined risks are clinically relevant.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.