fetching data ... 
Background: VEXAS (Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic) syndrome is a recently recognized, adult-onset autoinflammatory disease caused by somatic UBA1 gene mutations. Without population-wide screening, diagnosis relies on clinical suspicion and targeted genetic testing, making prevalence estimates highly dependent on patient selection. Reported prevalence, therefore, varies widely between population-based biobanks and clinically selected cohorts [1,2]. Few studies have evaluated the performance of targeted UBA1 testing or the epidemiology of VEXAS in real-world clinical settings, particularly in European populations.
Objectives: To evaluate a targeted screening strategy using predefined clinical and laboratory criteria to identify patients with suspected VEXAS syndrome referred to a Hematology center of a defined area in Northern Italy and eligible for UBA1 genetic testing, and to estimate the incidence and prevalence of VEXAS in the same area.
Methods: Figure 1 summarizes the predefined inclusion criteria for UBA1 genetic analysis. Male patients aged >45 years referred to the Hematology Unit of the defined area between 2019 and 2023 were retrospectively screened. Eligibility required persistent inflammation (CRP >0.5 mg/dL) and macrocytic anemia (hemoglobin <12 g/dL and mean corpuscular volume >95 fL). For computing the incidence rate, only patients residing in the definite area were included. Clinical and laboratory data were extracted from standardized electronic medical records and included inflammatory and systemic manifestations (e.g., fever, chondritis, vasculitis, deep venous thrombosis, skin manifestations, steroid dependence), hematological diagnoses, and the presence of vacuoles in bone marrow aspirates. Targeted UBA1 mutation testing was performed in patients with compatible clinical suspicion, bone marrow vacuoles, or both. Genetic analyses were conducted using Sanger sequencing on bone marrow aspirates, biopsies, or peripheral blood, when available, at the time of first suspicion. Study data were linked with regional demographic records to estimate the incidence and prevalence of VEXAS syndrome among male residents of the defined area aged > 45 years.
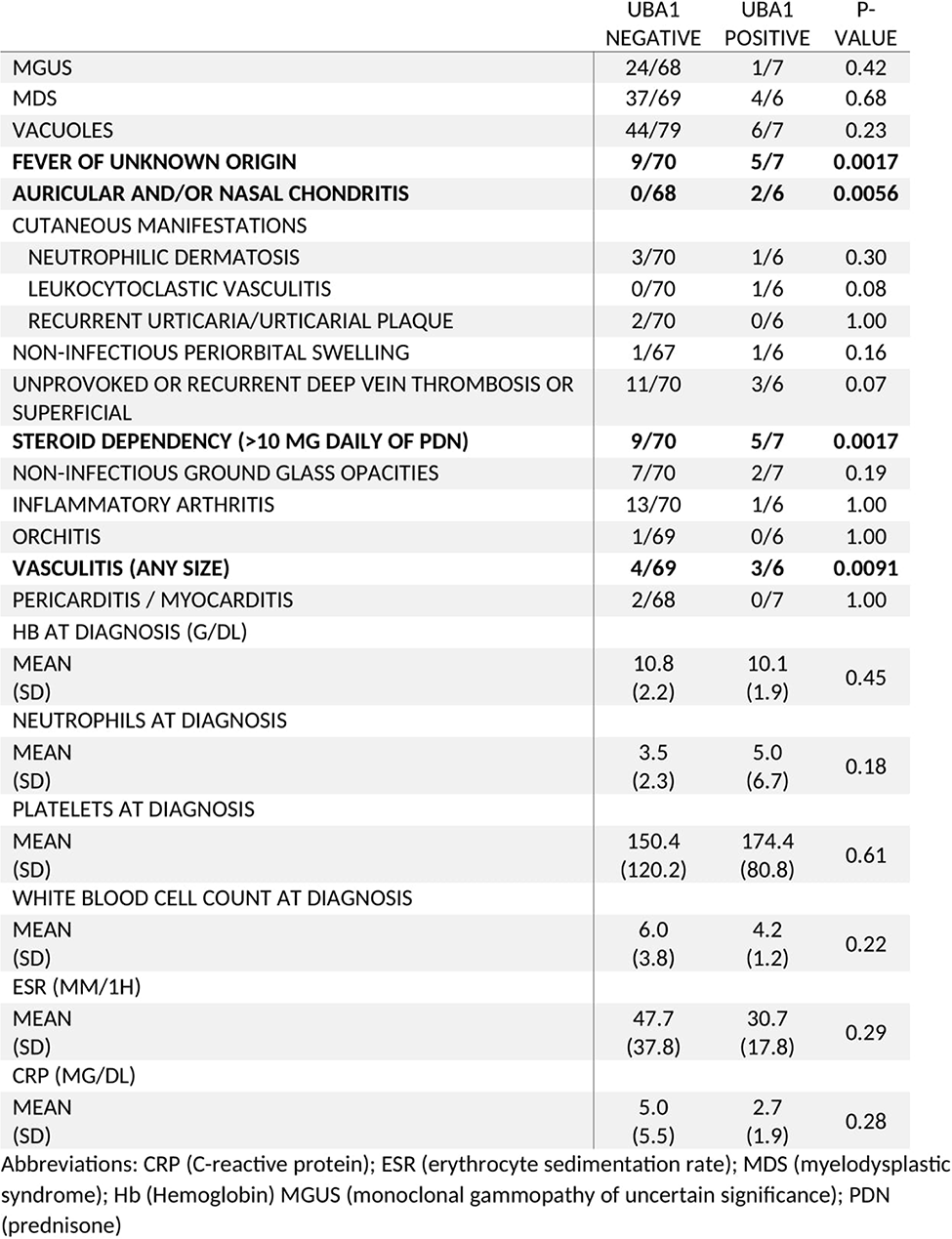
Results: A total of 88 patients were tested for a UBA1 mutation; 3 patients were excluded due to unavailable samples (Figure 1). Overall, 7/85 (8.2%) carried a pathogenic UBA1 variant, including 5 canonical variants (2 with p.Met41Thr and 3 with p.Met41Val), 1 pathogenic splice-site variant (c.118-1 G>C), and 1 variant of uncertain significance (c.177-36del, likely benign). 6/7 patients were diagnosed with VEXAS syndrome. Table 1 summarizes the clinical features of the patients. Mutation-positive individuals more often presented with fever of unknown origin (71%), steroid dependence (>10 mg prednisone/day, 71%), vasculitis (50%), and chondritis (33%). In contrast, laboratory parameters and hematological diagnoses showed minor differences, but the number of patients was too small to rule out chance. Combining clinical suspicion with bone marrow vacuoles yielded 85.7% sensitivity and 75.9% specificity for detecting UBA1 variants, outperforming either criterion alone (clinical suspicion: 100% sensitivity, 31.6% specificity; vacuoles: 85.7% sensitivity, 44.3% specificity). These findings support its use as a composite pre-test indicator for VEXAS screening. Among men aged >45 years, the estimated annual incidence of VEXAS syndrome was 0.63 per 100,000 (95% CI, 0.17–1.61), with a prevalence of diagnosed cases of 3.1 per 100,000 (95% CI, 0.8–7.9).
Conclusions: Although rare in the general population, VEXAS is relatively common in men >45 years with unexplained inflammation and macrocytic anemia, with an estimated incidence in the defined area of 0.63 per 100,000/year and a prevalence of diagnoses up to 2024 of 3.1 per 100,000. These figures are consistent with US and UK clinical cohorts but higher than those in unselected population datasets (1,2). Combining clinical suspicion with bone marrow vacuoles effectively identifies patients with pathogenic UBA1 variants and VEXAS syndrome, highlighting the value of targeted genetic testing in high-risk patients.
Flowchart of the selection process of the patients
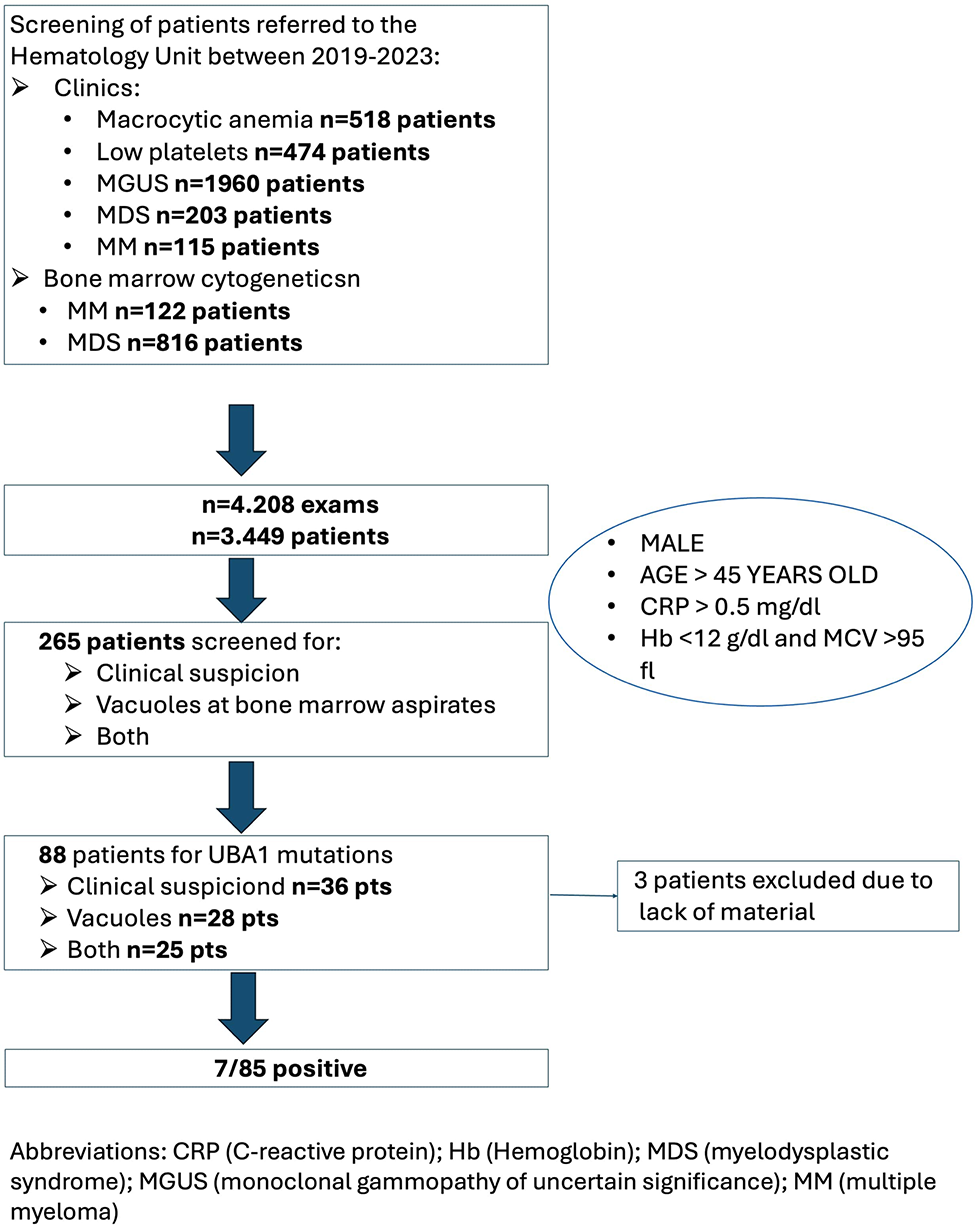
Table 1. Clinical features of patients involved
REFERENCES: [1] Beck DB, et al. Estimated Prevalence and Clinical Manifestations of UBA1 Variants Associated With VEXAS Syndrome in a Clinical Population. 2023 Jan 24;329(4):318-324. doi: 10.1001/jama.2022.24836.
[2] Martinez Rodriguez A, et al. Mapping VEXAS-associated and rare UBA1 variants in the United Kingdom: Insights from patient cohorts and the general population. Br J Haematol. 2025 May 25. doi: 10.1111/bjh.20176.
Acknowledgments: NIL.
Disclosure of Interests: None declared.