fetching data ... 
Background: VEXAS syndrome is a late-onset, UBA1-driven autoinflammatory disorder with substantial morbidity and a relevant risk of death. Determinants of fatal outcomes in real-world multicentre cohorts remain insufficiently characterised. In particular, whether mortality patterns differ across the main M41 variants and whether blood variant allele frequency (VAF) tracks fatal outcomes is uncertain.
Methods: Cross-sectional multicentre observational study including genetically confirmed VEXAS patients from 33 rheumatology units. UBA1 variants were grouped as M41T/M41L/M41V. Outcomes were overall mortality and adjudicated cause of death (VEXAS-related vs non–VEXAS-related). Blood VAF and treatment exposures were compared between survivors and deceased. Data are presented as n (%), mean (SD) and median (IQR).
Results: Fifty-six male patients with genetically confirmed VEXAS syndrome were included. Mean age at diagnosis was 72.13 (SD 9.36) years and the diagnostic delay was 44.5 (IQR 14.0–92.0) months. Baseline characteristics are described in Table 1.
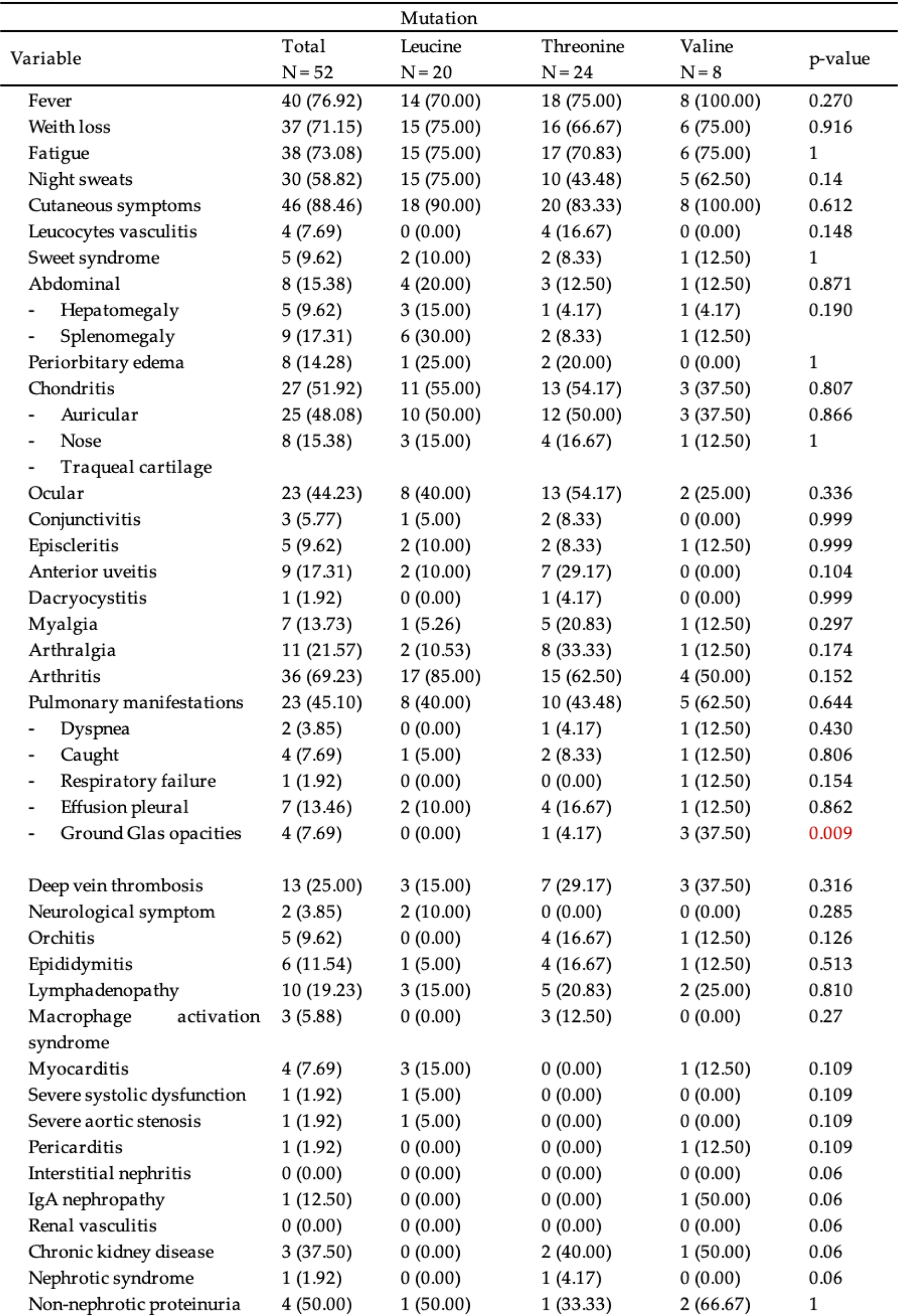
Among patients with M41 variants (n=52), the distribution was M41T n=24 (46.15%), M41L n=20 (38.46%), and M41V n=8 (15.38%). Overall mortality was n=14 (26.92%) M41L n=5 (25.00%), M41T n=7 (29.17%), M41V n=2 (25.00%). Across all deaths (n=14), VEXAS-related deaths were n=9 (64.29%) and non–VEXAS-related deaths n=5 (35.71%). VEXAS-related mortality accounted for n=4 (80.00%) in M41L, n=3 (42.86%) in M41T, and n=2 (100.00%) in M41V (p=0.336), indicating that all observed deaths in M41V were VEXAS-attributed.
M41V showed shorter diagnosis delay diagnostic profile: time from symptom onset to diagnosis was 14.0 (IQR 7.0–27.0) months, compared with 51.5 (IQR 10.0–93.0) in M41T and 67.0 (IQR 30.0–103.0) in M41L (p=0.105).
Patients with VEXAS related deathstended to have a shorter diagnostic delay (57.0 (IQR 33.0–81.0) vs 148.0 (IQR 131.0–154.0) months; p=0.060) and a lower age at diagnosis (mean 73.22 [SD 5.70] vs 80.40 [SD 9.32] years; p=0.181) compared with non–VEXAS-related deaths.
On the other hand, blood VAF was available in n=16 (32.65%); median VAF was 70 (IQR 40–80). VAF did not differ between survivors and deceased patients (p=0.550), but was numerically lower in those who died (mean 54.90 [SD 29.84] vs 62.28 [SD 22.57]; median 55 (IQR 34–76) vs 70 (IQR 40–80)), suggesting that fatal outcomes may not be driven by higher clonal burden in this cohort.
Regarding to treatment glucocorticoid exposure was identical in survivors vs deceased (39 (92.86%) vs 13 (92.86%), p >0.999), while escalation therapies were more frequent in deceased patients: MMF 4 (28.57%) vs 3 (7.69%) ( p =0.070). Notably, anti-IL6 and sulfasalazine were used only in deceased patients (2 (14.29%) each vs 0 (0.00%) in survivors; p =0.066 for both).
Conclusions: In this real-world multicentre cross-sectional cohort, mortality was frequent and predominantly VEXAS-related. A shorter diagnostic delay, particularly in M41V, appeared to mark a more aggressive trajectory, with deaths in M41V being uniformly VEXAS-attributed. Blood VAF was not associated with mortality and tended to be lower in fatal cases. Despite identical glucocorticoid exposure, escalation therapies were more frequent among deceased patients, supporting disease severity rather than higher clonal burden as the main signal linked to fatal outcomes.
Table 1. Baseline characteristics of patients with UBA1 M41 variants (M41T, M41L and M41V)
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.