fetching data ... 
Background: Chronic recurrent multifocal osteomyelitis (CRMO) is a rare autoinflammatory bone disorder characterised by sterile, recurrent bone inflammation with multifocal involvement. It represents part of the spectrum of autoinflammatory bone disorders (ABD) or osteopathies, where dysregulation of the innate immune system—particularly involving IL-1 and IL-10 imbalance, leading to NLRP3 inflammasome overactivation, which drives osteoclast activation and bone remodelling in the absence of bacterial infection. ABDs can be sporadic or monogenic. CRMO represents one of the sporadic forms and with growing recognition of the condition itself, its nomenclature has been suggested to be modified to chronic non-bacterial osteomyelitis (CNO). Globally, CRMO predominates in children and adolescents with peak onset between 7–12 years, affecting females more commonly than males. The highest reported incidence is from Western Europe, though true epidemiological data remain sparse due to underdiagnosis and limited global surveillance. In India, CRMO remains substantially underrecognised, with the literature confined to small case series describing 6–20 patients each, predominantly documenting diagnostic delays and treatment responses. No large-scale single-centre Indian study has systematically characterised the clinical phenotype, anatomical distribution, inflammatory profile, and imaging outcomes in this population. This creates a knowledge gap regarding whether CRMO presentation differs between geographic populations.
Objectives: To characterise the clinical, laboratory, radiological and therapeutic profile of children with CRMO in a South-Indian single-centre cohort, documenting site-specific involvement patterns, inflammatory markers, treatment utilisation, and 1-year imaging outcomes (where available).
Methods: Retrospective cohort study of children diagnosed with CRMO between January 2015 and December 2025 at a tertiary paediatric rheumatology centre in Kerala, South India. Bristol criteria (2012) was used for classifying patients. Consecutive patients were included if they had: (i) insidious onset bone pain and/or swelling, (ii) multifocal osteitis on whole-body MRI compatible with non-infectious osteomyelitis, and (iii) exclusion of infectious, malignant, and metabolic causes; sterile bone biopsy demonstrating chronic inflammation was obtained in diagnostically uncertain or atypical cases (44.7%). Demographic data (age, sex), duration of symptoms prior to diagnosis, comorbid autoimmune/autoinflammatory diseases, HLA-B27 status, inflammatory markers (CRP, ESR), and detailed MRI-based anatomical distribution (vertebral, mandibular, isolated vs multifocal) were systematically extracted. Treatment exposure to bisphosphonates, methotrexate, sulphasalazine, and JAKi/bDMARDs was recorded, along with the proportion receiving combination regimens. One-year follow-up MRI, when available, was used to classify outcomes as complete resolution, persistent lesions, or new lesions, and to estimate rates of radiological remission and disease stabilisation in the treated cohort.
Results: Of the 103 children included (52 boys, 51 girls), the mean age at presentation was 10.9 years (range 4.5–18.16), with a mean symptom duration of 13.49 months (range 1–70). Comorbid conditions were documented in 34 patients (33%), most frequently psoriasis spectrum disorders (12) and juvenile idiopathic arthritis spectrum (4), with the remainder comprising other autoimmune or autoinflammatory diagnoses.
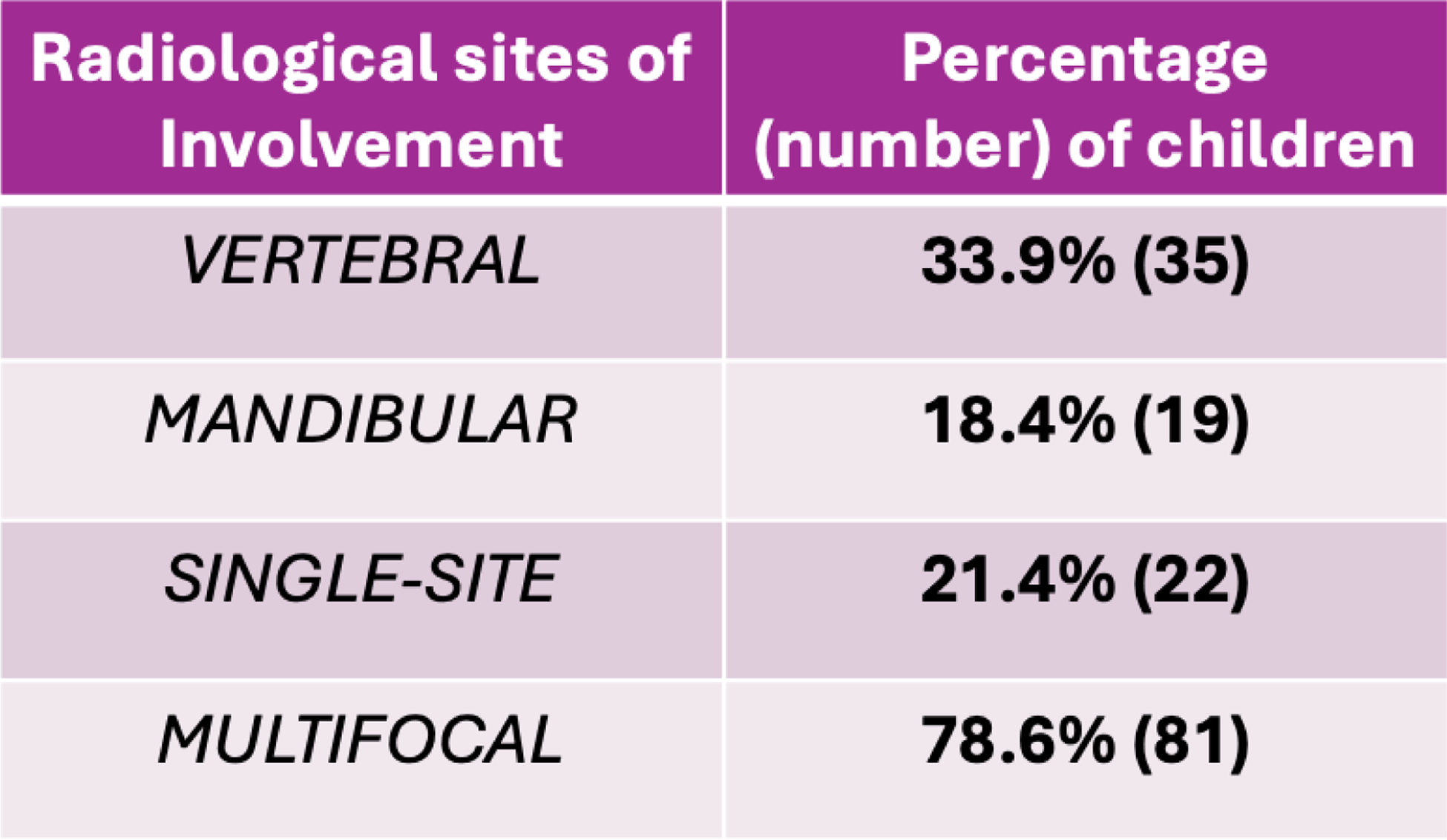
Whole-body MRI demonstrated multifocal disease in 81 children (78.6%), with vertebral involvement in 35 (33.9%) and mandibular involvement in 19 (18.4%). Isolated single-site osteitis was seen in 22 patients (21.4%), of whom more than half (12/22, 11.7% of the total cohort) had isolated mandibular disease. HLA-B27 testing was performed in 43 patients (41.7%), with only 3 children (7.0% of those tested) returning a positive result, supporting a predominantly HLA-B27–negative autoinflammatory phenotype. Inflammatory markers at presentation were heterogeneous, with a mean CRP of 10.99 mg/L and mean ESR of 38.42 mm/hr, frequently showing poor concordance with overall severity.
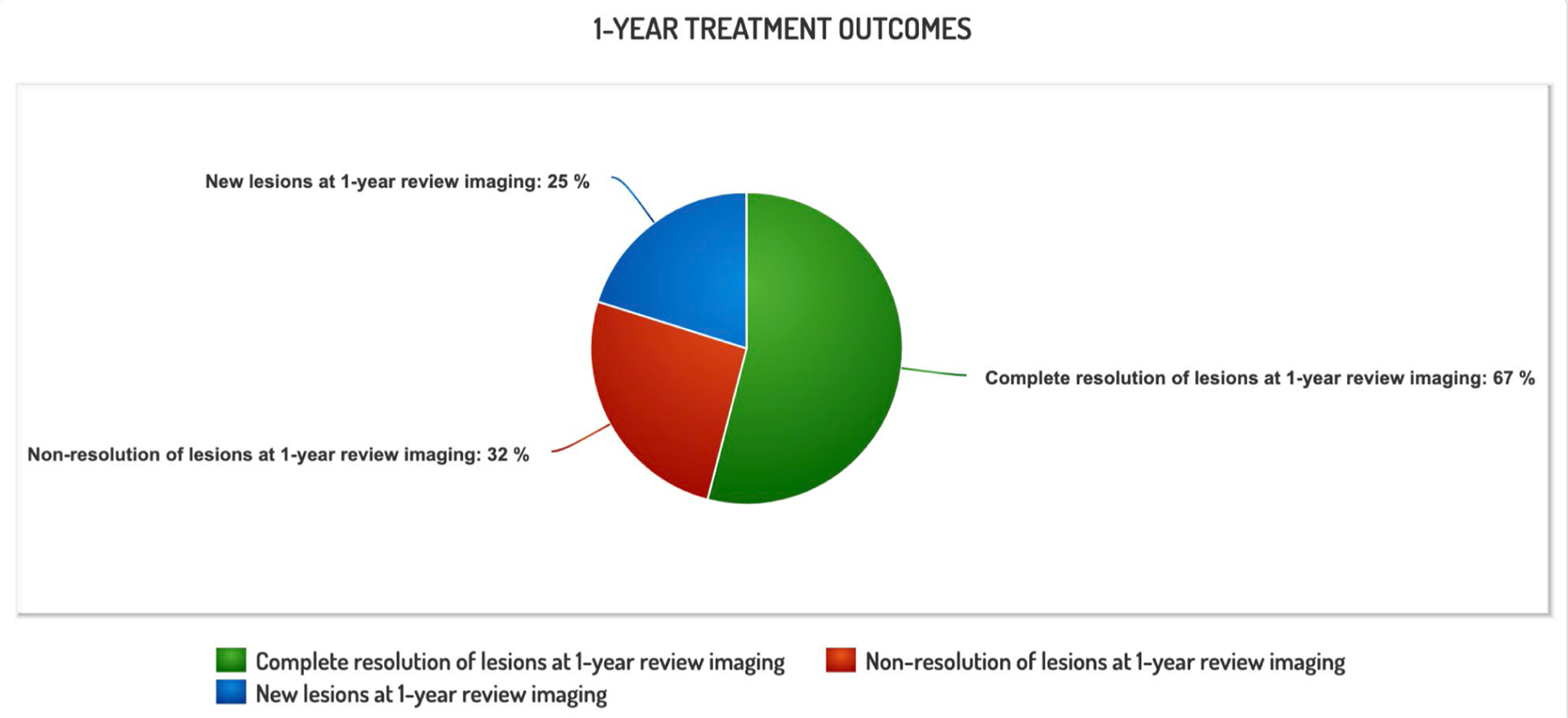
Bisphosphonates were used in 70 patients (67.9%), methotrexate in 52 (50.5%), and sulphasalazine in 13 (12.6%), while 7 children (6.8%) required escalation to targeted therapy with JAK inhibitors and/or biologic DMARDs; 32 patients (31.0%) received combined bisphosphonate–methotrexate regimens. Bone biopsy was undertaken in 46 patients (44.7%), uniformly demonstrating sterile chronic inflammatory changes. Among the 62 children (60.2% of the cohort) who underwent follow-up MRI at 1 year, 42 (67.7% of those imaged; 40.7% of the total cohort) showed complete radiological resolution of lesions, 20 (32.3%; 19.4% of total) had persistent lesions without complete remission, and 16 (25.8%; 15.5% of total) developed new lesions despite therapy. Overall, 46 children (44.7% of the entire cohort) exhibited no new lesions at 1 year, indicating radiological disease stabilisation in nearly half of the patients under follow-up.
Conclusions: This largest single-centre Indian CRMO cohort demonstrates a South-Asian phenotype characterised by substantial vertebral and mandibular involvement, near-equal sex distribution, and a 33% comorbidity burden. The 67.7% complete resolution rate at 1 year with bisphosphonate-MTX combination therapy provides encouraging evidence for conventional immunosuppressive strategies in this population. However, 25-32% with persistent or new lesions highlights the need for earlier diagnosis , standardised treatment protocols , and prospective outcome studies to optimise disease management in resource-limited settings. Mean symptom duration of 13.49 months prior to diagnosis is concerning and highlights a knowledge gap when it comes to ABDs. This series underscores CRMO as a significant but overlooked autoinflammatory diagnosis in childhood rheumatology in India.
Table 1.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.