fetching data ... 
Background: Anti-neutrophil cytoplasmic antibody–associated vasculitides (AAV) are rare autoimmune diseases with significant morbidity and mortality [1]. Rituximab (RTX) is the current standard of care for granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA) [2,3]. However, RTX may induce hypogammaglobulinemia (Hγ), sometimes prolonged [4], leading to infectious complications. The incidence of post-RTX Hγ appears higher in AAV than in other autoimmune diseases [5]. While transient Hγ is well described, the persistence of this deficit remains poorly understood [6], as do its potential links with primary immunodeficiencies (PID), such as common variable immunodeficiency (CVID) [7].
Objectives: The national multicenter DIVA study aimed to characterize AAV patients who developed prolonged hypogammaglobulinemia after RTX through a retrospective cohort analysis complemented by a prospective standardized immunological evaluation.
Methods: This cohort was compared with two control groups: AAV patients without prolonged Hγ and a well-characterized national cohort of CVID patients from the CEREDIH registry (French National Reference Center for Primary Immunodeficiencies).
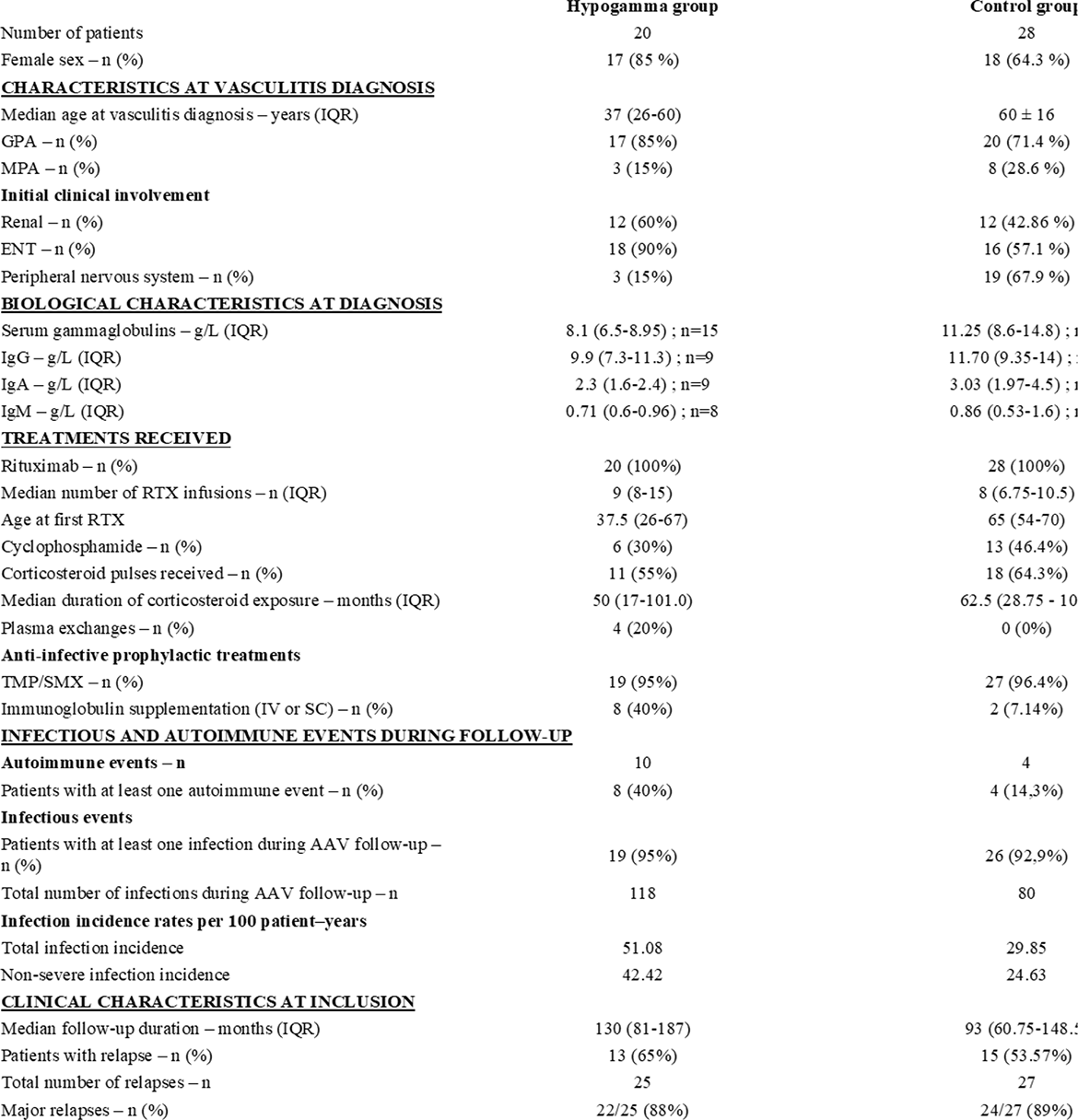
Results: 20 patients were included. The median time to Hγ onset was 15 months (6–33) after the first RTX exposure, and hypogammaglobulinemia persisted after a median follow-up of 82 months (60–127). The median age at Hγ diagnosis was 40 years (29–54). Compared with AAV patients without prolonged Hγ, the prolonged Hγ group had a higher rate of non-severe infections ( p=0.0007 ) and a significantly younger age at diagnosis (37 years, p=0.0023 ).
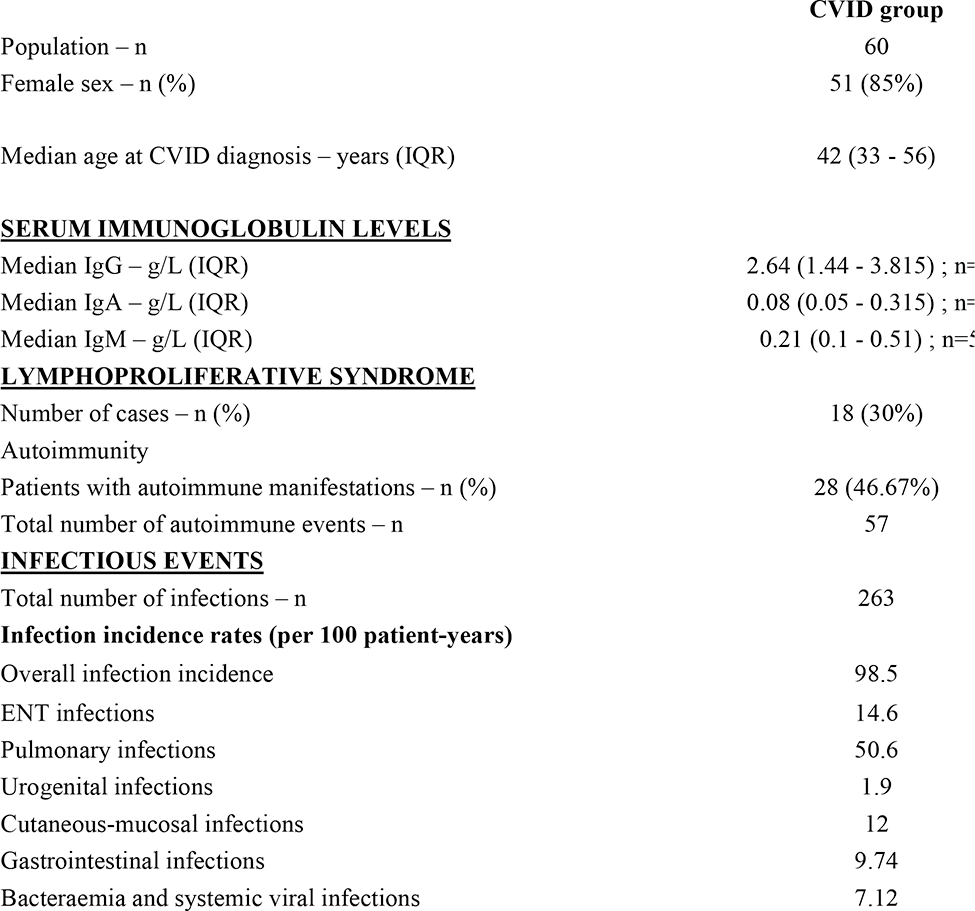
Comparison with CEREDIH CVID patients revealed similar age at diagnosis, overlapping immunoglobulin levels, and comparable infectious and autoimmune profiles.
Conclusions: To our knowledge, this is the first study to compare prolonged RTX-induced hypogammaglobulinemia in AAV with common variable immunodeficiency. Prolonged RTX-induced hypogammaglobulinemia represents a lasting and severe complication sharing features with CVID. Systematic immunoglobulin screening, particularly in younger patients, and comprehensive immunological evaluation are warranted to better define this secondary immunodeficiency.
Table 1 .
REFERENCES: [1] Terrier B et al. Orphanet J Rare Dis. 2020;15:351.
[2] Guillevin L et al. N Engl J Med. 2014;371:1771-80.
[3] Stone JH et al. N Engl J Med. 2010;363:221-32.
[4] Kacar M et al. BioDrugs. 2025;39:103-30.
[5] Kridin K et al. Autoimmun Rev. 2020;19:102466.
[6] Liberatore J et al. J Autoimmun. 2024;142:103130.
[7] Ottaviano G et al. J Allergy Clin Immunol Pract. 2020;8:273-82.
Acknowledgments: NIL.
Disclosure of Interests: None declared.