fetching data ... 
Background: Complementary to FRAX, FRAXplus incorporates additional risk factor information to adjust estimates of 10-year probabilities for major osteoporotic (MOF) and hip fractures.
Objectives: We aimed to determine which of the FRAXplus adjustments would be the main drivers of increased (or decreased) fracture risk, and how they would affect risk classification and thereby treatment recommendations in Switzerland.
Methods: This study analysed prospective data from the Swiss Osteoporosis Registry (2015–2023), which includes all standard FRAX variables, as well as lumbar spine bone mineral density (LS-BMD), trabecular bone score (TBS), fall history in previous year, glucocorticoid dosages, and location and recency of prior fractures. Data on hip axis length and type 2 diabetes duration were not available.
Results: A total of 28,708 individuals were included. The median 10-year fracture probability for MOF was 16 % [IQR: 9; 24] using standard FRAX and 18% [IQR: 11, 28] with FRAXplus adjustments. Most individuals (72%) had a higher probability using FRAXplus adjustments (mean absolute increase: +4.8%), while 27% had a lower probability (mean absolute decrease: –1.0%). The difference between lumbar spine and femoral neck T-scores (LS–FN), and TBS had the broadest impact, being available for adjustment in the majority of individuals and therefore influencing nearly all fracture risk estimates. However, the magnitude of change (expressed as a percentage of the baseline FRAX probability) was generally modest for LS–FN and TBS, and adjustments for higher glucocorticoid doses were likewise small. On an individual level, ≥1 fall and recent fractures, particularly vertebral or hip fractures, were the strongest drivers of increased fracture probability. Applying FRAXplus adjustments with Swiss thresholds led to upward reclassification in 16% of MOF and 2% of hip fracture estimates, and downward reclassification in 1% and 0.2%, respectively.
Conclusions: FRAXplus adjustments significantly alter fracture risk estimates in most individuals. While LS–BMD and TBS consistently influence outcomes, vertebral and hip fractures and falls are the most impactful on an individual level. These shifts meaningfully affect treatment recommendations according to Swiss clinical guidelines.
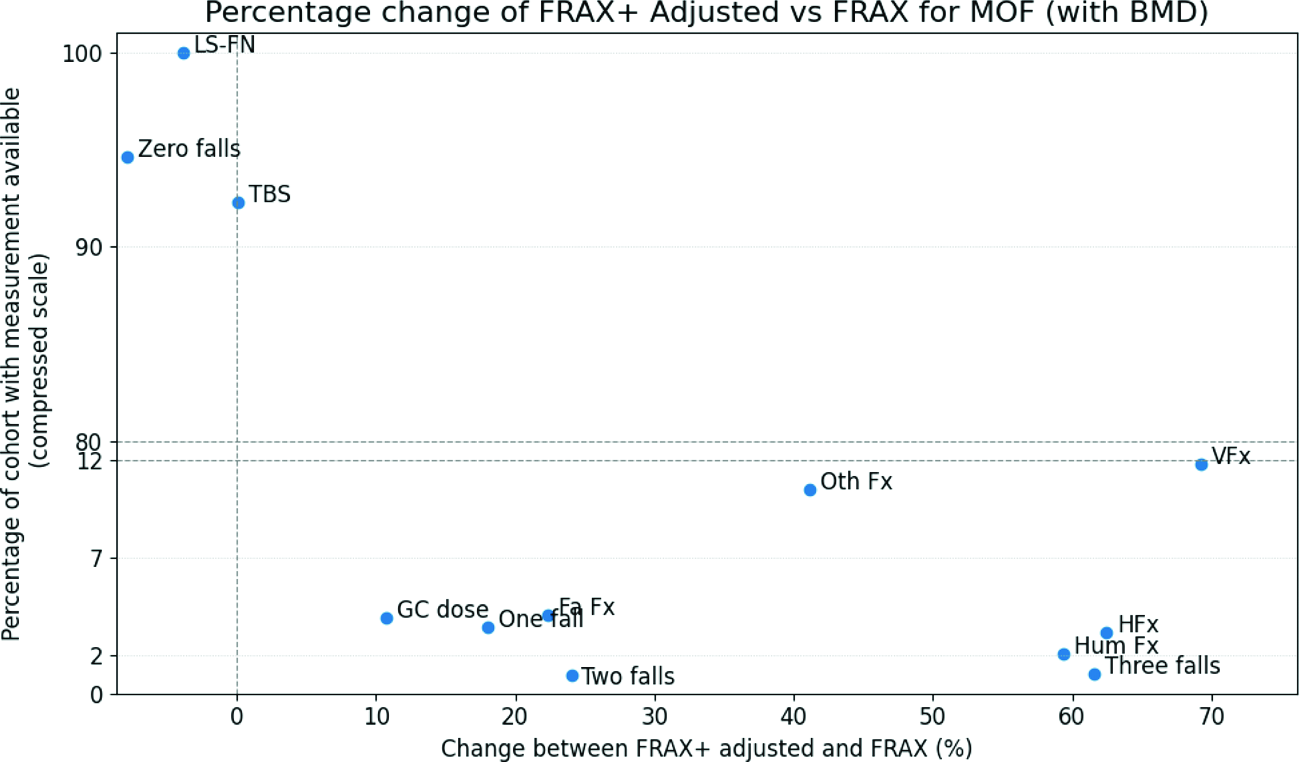
Mean percentage change between FRAXplus adjusted and standard FRAX values, depending on the variable and its impact on the number of individuals included in the 10-year MOF probability estimation (with BMD).
Abbreviations: LS-FN: difference between lumbar spine and femoral neck BMD, TBS: Trabecular Bone Score, GC: Glucocorticoids, Fx: Recent fracture (FA: Forearm, Oth: Other, H: Hip fracture, Hum: Humerus fracture, V: Vertebral fractures)
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.