fetching data ... 
Background: Home-based telerheumatology is a well-established approach to improve access to care for patients with rheumatic and musculoskeletal diseases. However, a recent randomized clinical trial (RCT) showed that in-person visits may be preferred by many rheumatology patients. Thus, it is key to understand factors influencing patient acceptability of telerheumatology.
Objectives: We aimed to identify demographic, socioeconomic, and disease-specific factors associated with patient acceptability of home-based telerheumatology.
Methods: We utilized data from an RCT (NCT04704544) conducted between August 2021 and January 2023 at two U.S. academic medical centers. The RCT compared patient satisfaction with home-based telerheumatology versus in-person care. Eligible participants were adults with a rheumatic condition and 2 or more rheumatology clinic visits within the prior 18 months. Participants enrolled in the RCT were randomized to receive either a telerheumatology visit or an in-person visit for their next rheumatology appointment, and then assigned to the other type of visit for their subsequent appointment. Outcomes were assessed via phone surveys after each visit. Patient acceptability of telerheumatology was assessed using a 17-item validated questionnaire, the Telemedicine Perception Questionnaire (TMPQ). TMPQ measures usefulness, reliability, ease of use, interaction quality, and satisfaction with services received via telemedicine, with possible scores from 17 to 85 (highest scores represent higher acceptability of telemedicine). This analysis includes data collected after each of the two rheumatology appointments occurring as part of the RCT. Because a telerheumatology visit occurred at only one rheumatology appointment by design, each participant contributed a single TMPQ score collected after their telerheumatology visit (i.e., the first visit if randomized to telerheumatology first; the second visit if telerheumatology occurred at the subsequent visit). We excluded data from patients answering <50% of the TMPQ questions. For participants with <50% missing data on the TMPQ, we used the patient’s mean score for answered questions, scaled to the full scale of items (i.e., sum of items answered multiplied by 17 divided by the number of questions answered). Satisfaction with telemedicine visit was rated 0 to 10 satisfaction scale, with higher scores associated with higher satisfaction. Our independent variables (see Table 1 footnote for details), were age, sex, race, telemedicine visit type (audio-only vs video), geocoded distance from patient’s home to clinic, education level (≥4 years degree vs ≤some college), health literacy (adequate vs inadequate), medication adherence (adherent vs non-adherent), medication type, and disease condition. We used frequencies (proportions) to describe categorical variables and means (SD) for continuous variables. We created univariable and multivariable linear regression models to analyze the association between independent variables and telerheumatology acceptability measured using TMPQ. We generated a full model including all independent variables, then used the backward selection to remove variables that were not found to be statistically significant, while keeping in those variables with biological significance or clinical rationale. Statistical significance was defined as p ≤0.05.
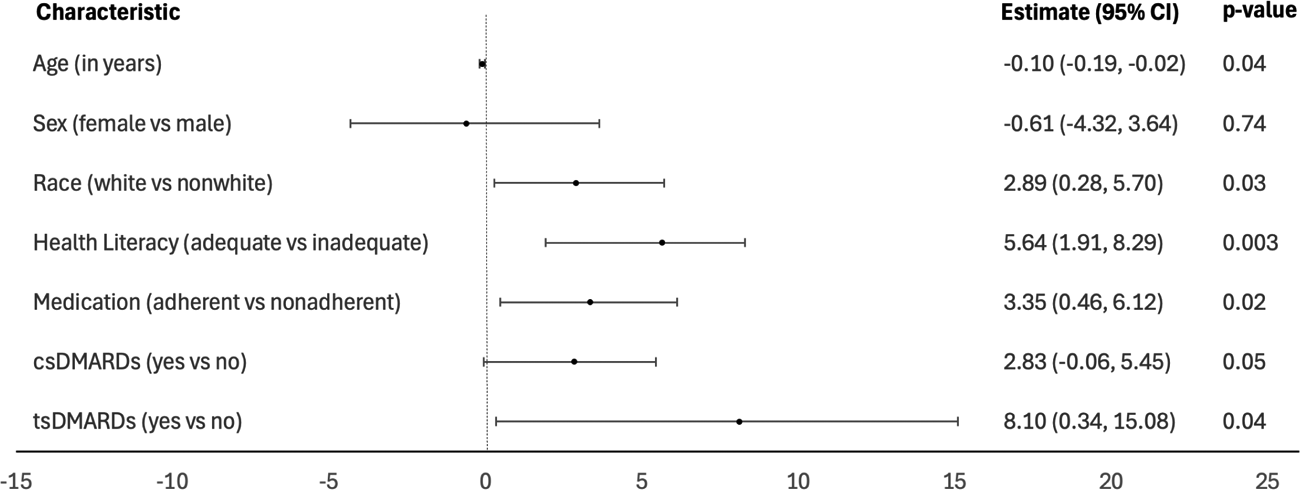
Results: We analyzed data from 266 patients who had telerheumatology visits and available TMPQ scores. Our study population included 84.96% female and 50.38% White patients. The mean (SD) age was 54.38 (14.08) years ( Table 1 ). Approximately 78% of the patients rated their visit ≥9 (high satisfaction), and the mean (SD) TMPQ score was 65.05 (10.58). We found a weak positive relationship between satisfaction and TMPQ (Pearson correlation coefficient = 0.33). In univariable analysis, White (vs other) race (p=0.01), adequate (vs. inadequate) health literacy (p=0.002), and use of conventional synthetic disease-modifying antirheumatic drugs (DMARDs) (p=0.02) were significantly associated with higher TMPQ scores. Multivariable linear regression ( Table 2 ) showed that younger age (95% CI -0.19, -0.02, p=0.04), White race (95% CI 0.28, 5.70, p=0.03), adequate health literacy (95% CI 1.91, 8.29, p=0.003), high medication adherence (95% CI 0.46, 6.12, p=0.02), and use of conventional synthetic DMARDs (95% CI -0.06, 5.45, p=0.05) and targeted synthetic DMARDs (95% CI 0.34, 15.08, p=0.04) were associated with higher TMPQ scores.
Conclusions: In our study, several patient characteristics were directly associated with telerheumatology acceptability, including younger age, White race, adequate health literacy, high medication adherence, and use of conventional and targeted synthetic DMARDs. Our findings can help clinicians determine which patients might be receptive to telerheumatology and will inform future studies focused on creating interventions to mitigate low telerheumatology acceptability.
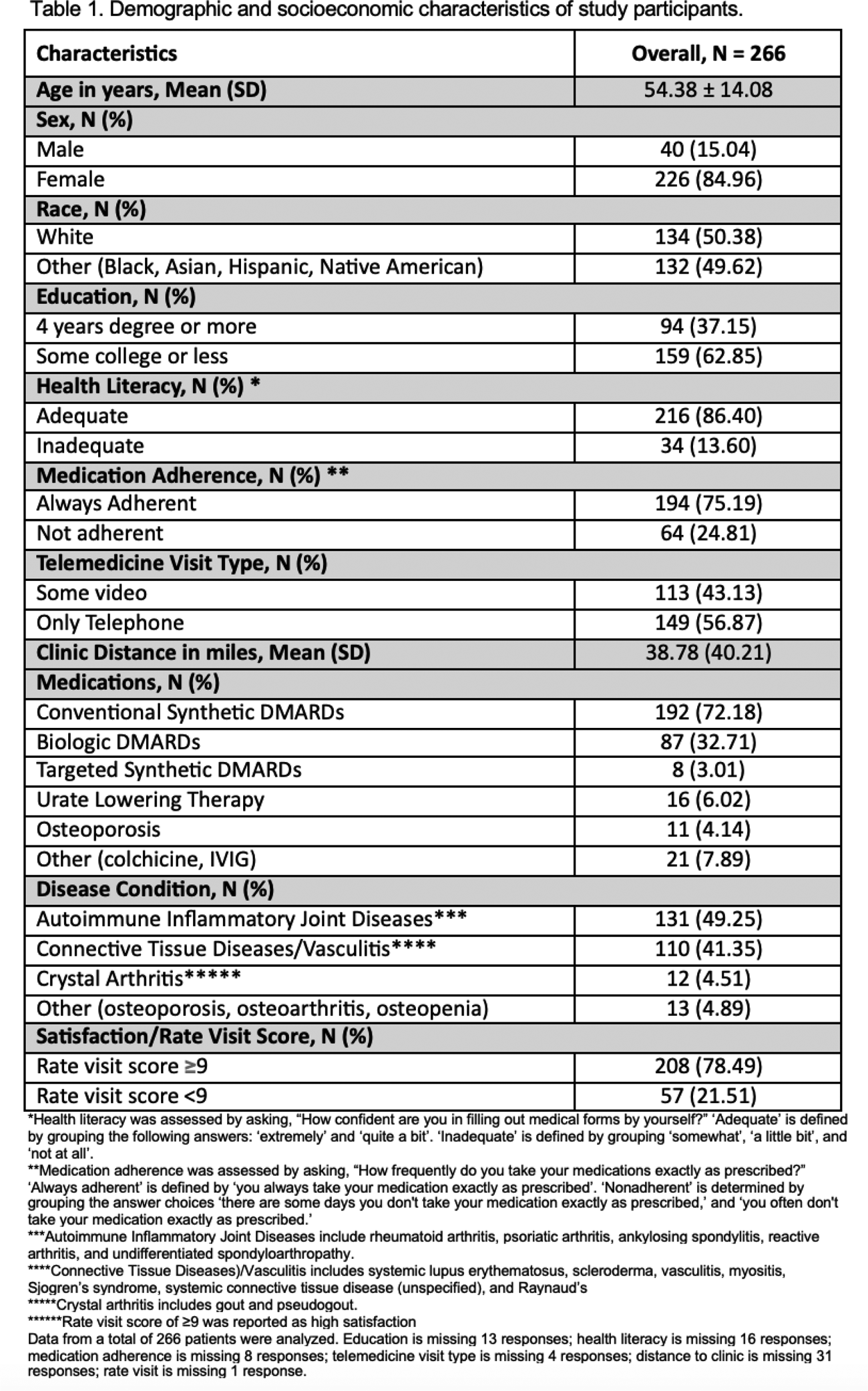
Table 2. Multivariable linear regression analysis of factors associated with the acceptability of telemedicine using the TMPQ score. p≤0.05 represents statistical significance.
REFERENCES: [1] Jackson LE, Yazdany J, Leach JM, Saag KG, Aaron K, Curtis JR, Goglin S, Margaretten M, Chae DH, Paez D, Cutter G. Satisfaction with telemedicine versus in-person visits in rheumatology: a noninferiority randomised controlled trial. Annals of the Rheumatic Diseases. 2025 May 8.
Acknowledgments: NIL.
Disclosure of Interests: Hareem Farooq: None declared, Lesley Jackson: None declared, Rahima Begum: None declared, Gary Cutter Data and Safety Monitoring Boards: Applied Therapeutics, AI therapeutics, AMO Pharma, Argenx, Astra-Zeneca, Avexis Pharmaceuticals, Bristol Meyers Squibb, CSL Behring, Cynata Therapeutics, DiamedicaTherapeutics, Horizon Pharmaceuticals, Immunic, Inhibrix, Karuna Therapeutics, Kezar Life Sciences, Medtronic, Merck, Meiji Seika Pharma, Mitsubishi Tanabe Pharma Holdings, Prothena Biosciences, Novartis, Pipeline Therapeutics (Contineum), Regeneron, Sanofi-Aventis, Teva Pharmaceuticals, United BioSource LLC, University of Texas Southwestern, Zenas BioPharma. Consulting or Advisory Boards: Alexion, Antisense Therapeutics/Percheron, Avotres, Biogen, Clene Nanomedicine, Clinical Trial Solutions LLC, Endra Life Sciences, Cognito Therapeutics, Genzyme, Genentech, Immunic, Klein-Buendel Incorporated, Kyverna Therapeutics, Inc., Linical, Merck/Serono, Noema, Neurogenesis, Perception Neurosciences, Protalix Biotherapeutics, Regeneron, Revelstone Consulting, Roche, SAB Biotherapeutics, Sapience Therapeutics, Scott&Scott LLP, Tenmile. Dr. Cutter is employed by the University of Alabama at Birmingham and President of Pythagoras, Inc. a private consulting company located in Birmingham AL., Kenneth Saag Arthrosi (Consultant); Atom Bioscience (Consultant); Cyrstalys (Consultant); LG Pharma (Consultant); Novo Nordisc (Consultant); Shanton (Consultant); Sobi (Consultant), Arthrosi (Grant/Research Support); Inventis (Grant/Research Support); LG Pharma (Grant/Research Support); Olatec (Grant/Research Support), Jinoos Yazdany Pfizer (Consultant); UCB (Consultant), AstraZeneca (Consultant, Grant/Research Support); Aurinia (Grant/Research Support); BMS Foundation (Grant/Research Support, BMS Foundation); Gilead (Grant/Research Support), Maria Danila Boehringer-Ingelheim (Consultant).