fetching data ... 
Background: Pregnancy in women with autoimmune rheumatic diseases (ARDs), including systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), rheumatoid arthritis (RA), and Sjögren’s syndrome, is associated with a high burden of adverse pregnancy outcomes (APOs) driven by immune-mediated inflammation, thrombosis, and placental dysfunction. Conventional clinical risk factors only partially explain this heterogeneity, limiting early identification of high-risk patients.
Objectives: We hypothesized that obstetric complications in ARDs are best predicted by an integrated immune-clinical risk model that combines autoantibody, inflammatory, and disease-activity biomarkers.
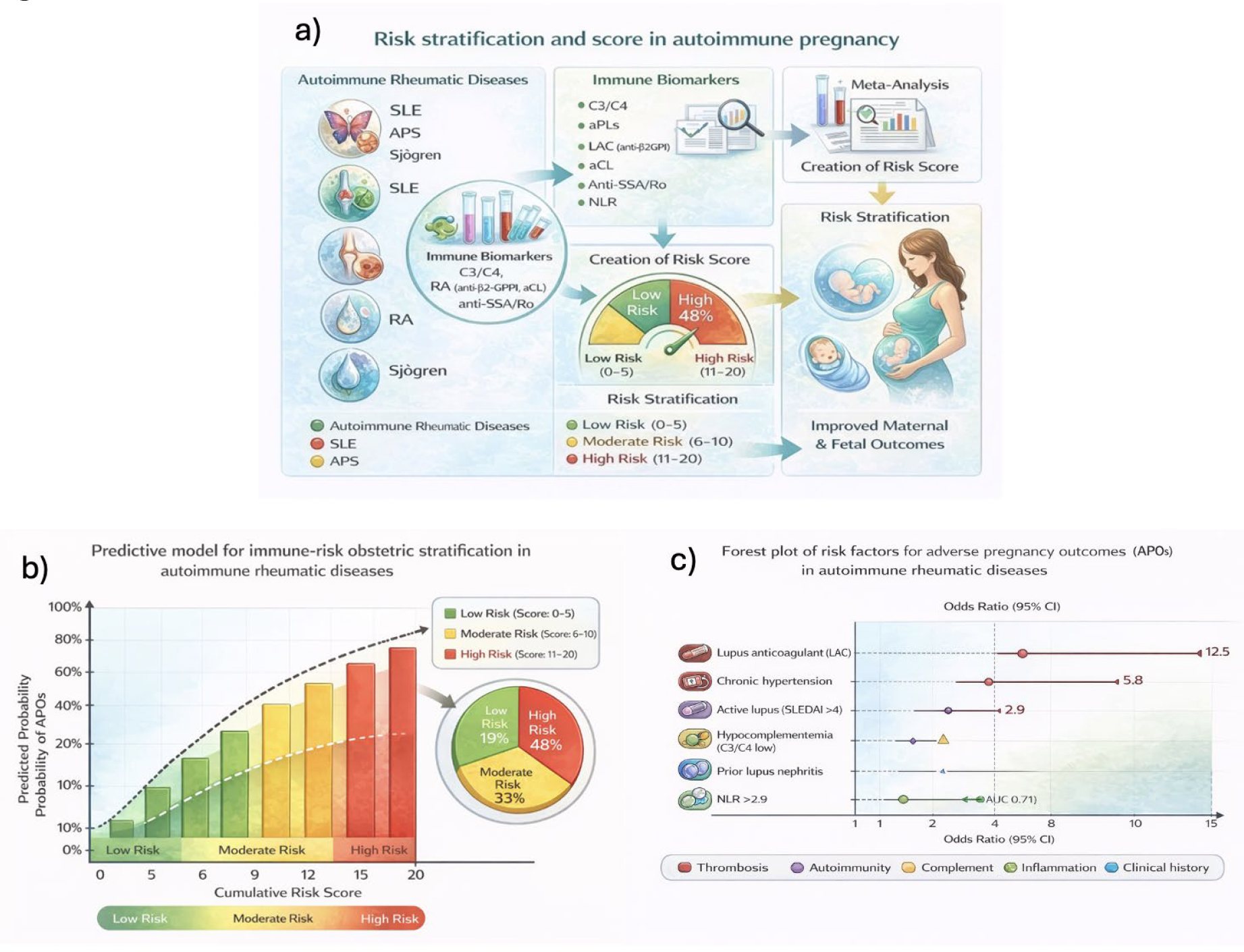
Methods: A systematic review and meta-analysis were conducted across PubMed, Embase, Web of Science, and Scopus to identify biomarkers and clinical predictors of APOs in pregnant women with ARDs. More than 150 studies were included. Extracted variables comprised lupus anticoagulant (LAC), anti-β2-glycoprotein I, anticardiolipin antibodies, complement activation (C3, C4, sC5b-9), neutrophil-to-lymphocyte ratio (NLR), anti-SSA/Ro, disease activity indices (SLEDAI, DAS28), and key clinical factors (nephritis, chronic hypertension, prior pregnancy loss). Effect sizes were pooled using random-effects meta-analysis and translated into weighted predictors within a point-based risk calculator, generating cumulative scores for individual patient stratification.
Results: The final model integrated 12 high-evidence immune and clinical predictors of APOs. LAC emerged as the strongest risk factor for pregnancy loss after 12 weeks (OR ≈ 12.5), while chronic hypertension conferred a high risk for preeclampsia (OR 5.8). Active lupus (SLEDAI >4) was associated with increased preterm birth risk (OR 2.9), and both prior nephritis and hypocomplementemia significantly amplified adverse outcome probability, reflecting immune-complex-driven placental injury (Figure 1). Inflammatory activation captured by NLR >2.9 showed moderate predictive capacity for maternal–fetal complications (AUC 0.71). Integration of these variables into a cumulative score enabled stratification of patients into low-, moderate-, and high-risk categories. Internal validation demonstrated 81% sensitivity and 74% specificity for predicting APOs.
Conclusions: We developed an evidence-based, biomarker-driven risk stratification model that captures the immune-mediated mechanisms underlying obstetric complications in autoimmune rheumatic diseases. By integrating autoantibody profiles, complement activation, inflammation, and disease activity, this tool provides a precision-based framework for early identification of high-risk pregnancies. This predictive model supports a shift from symptom-based to immune-based obstetric risk assessment in rheumatology and provides a foundation for personalized monitoring and intervention strategies in women with ARDs.
Predictive Biomarkers and Clinical Variables Included in the Obstetric Risk Stratification Model for Autoimmune Rheumatic Diseases
| Predictor | Effect Size (OR) | Clinical Interpretation |
|---|---|---|
| Lupus anticoagulant (LAC) | ~12.5 | Strongest predictor of adverse pregnancy outcomes |
| Chronic hypertension | 5.8 | Strong risk factor for preeclampsia |
| Active lupus (SLEDAI >4) | 2.9 | Associated with preterm birth |
| Prior lupus nephritis | ↑ | Increases APO risk, esp. with proteinuria |
| Hypocomplementemia (C3/C4 low) | ↑ | Reflects active immune complex deposition |
| NLR >2.9 | AUC = 0.71 | Predicts maternal-fetal complications |
| Anti-SSA/Ro positivity | -- | Indicates risk for fetal heart block, integrated if present |
| History of pregnancy loss | ↑ | Included as cumulative clinical risk |
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.