fetching data ... 
Background: Familial Mediterranean Fever (FMF) and gout are chronic auto-inflammatory disorders characterized by recurrent inflammatory attacks and long-term morbidity. Colchicine is the cornerstone of treatment for both conditions, effectively reducing inflammatory activity and preventing disease-related complications. Beyond its well-established anti-inflammatory properties, colchicine has been hypothesized to exert neuroprotective effects through modulation of microtubule dynamics, inhibition of inflammasome activation, and suppression of proinflammatory cytokines. However, the long-term cognitive impact of colchicine remains insufficiently studied, particularly in elderly patients with prolonged exposure.
Objectives: This study aimed to evaluate neurocognitive performance in patients with Familial Mediterranean Fever and gout receiving long-term colchicine therapy, and to compare cognitive outcomes with those of healthy controls. Additionally, we sought to determine whether disease duration, inflammatory burden, or colchicine exposure influenced cognitive performance.
Methods: This cross-sectional study included 23 patients with FMF, 19 patients with gout, and 24 age-matched healthy controls aged ≥60 years. All patients had been receiving regular colchicine therapy for at least six months. Demographic data, clinical characteristics, disease duration, and treatment parameters were recorded. Neurocognitive evaluation was performed using a comprehensive battery including the Wechsler Memory Scale (WMS), Stroop Test, verbal fluency tests, Benton Facial Recognition Test, Digit Span Test, and other standardized neuropsychological assessments. Cognitive domains assessed included attention, executive functions, working memory, visuospatial ability, and verbal memory. Statistical comparisons were performed between groups, and correlations with disease duration, colchicine exposure, and laboratory parameters were analyzed.
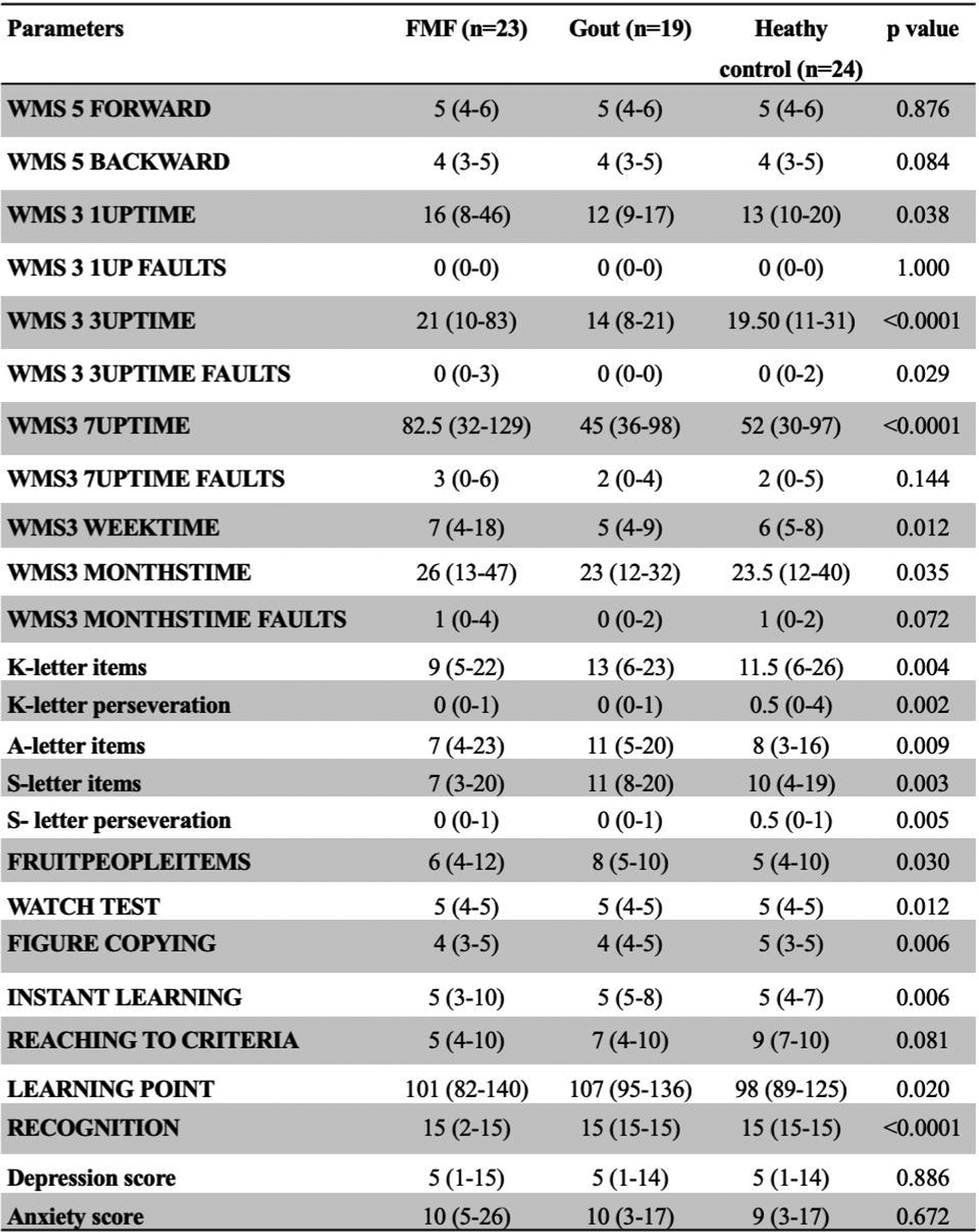
Results: A total of 66 participants were included (23 FMF, 19 gout, 24 controls). There were no significant differences among the groups in terms of age or sex distribution (p = 0.928 and p = 0.160, respectively) (Table 1). Educational level was lowest in the FMF group and highest in the healthy control group (p = 0.022). FMF patients had a significantly longer disease duration and longer cumulative colchicine exposure compared with the gout group (p<0.001). Patients with gout reported significantly higher rates of regular newspaper reading and news consumption and lower rates of smoking compared to the FMF group (p < 0.05 for all comparisons). The use of antidepressants was more frequent in the FMF group, whereas the use of anxiolytic medications did not differ significantly between groups (p = 0.076 and p = 0.548, respectively). Among comorbid conditions, hypertension was significantly more prevalent in the gout group (52.6% vs. 84.2%, p = 0.030). Baseline laboratory parameters, including complete blood count, routine biochemistry, and inflammatory markers, were comparable between groups, with the exception of serum uric acid levels, which were significantly higher in the gout group. Patients with FMF had a younger age at diagnosis and treatment initiation, a longer disease duration, longer cumulative colchicine exposure, and higher daily colchicine doses compared to patients with gout (all p < 0.001). The median time from symptom onset to initiation of colchicine therapy was significantly longer in the FMF group, with a median delay of 25 years, whereas most patients with gout initiated treatment within the same year of diagnosis (p < 0.0001). Detailed neurocognitive test results are presented in Table 2. Patients with FMF demonstrated significantly poorer performance in multiple domains including verbal learning, delayed recall, executive functions, and processing speed, compared with both gout patients and healthy controls. In contrast, gout patients showed performance largely comparable to controls across most cognitive domains.
Importantly, poorer neurocognitive performance correlated with longer disease duration and higher cumulative inflammatory burden, rather than with colchicine dose or treatment duration. No significant association was observed between cumulative colchicine exposure and cognitive impairment. On the contrary, patients receiving long-term colchicine did not demonstrate accelerated cognitive decline compared to controls. Depression and anxiety scores were similar across all groups and did not significantly confound cognitive outcomes.
Conclusions: This study demonstrates that long-term colchicine use does not adversely affect cognitive performance in patients with FMF or gout. Cognitive impairment observed in FMF appears to be more closely related to chronic inflammation and prolonged disease activity rather than colchicine exposure itself. These findings support the neurological safety of long-term colchicine therapy and suggest a potential protective effect against inflammation-related cognitive decline. Further prospective studies with larger cohorts are warranted to clarify the neuroprotective potential of colchicine and to explore its role in modulating neuroinflammatory pathways.
Table 1. Baseline characteristics of the study groups

Table 2. Results of neurocognitive evaluation according to test domains
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.