fetching data ... 
Background: The UK General Medical Council recommends that curriculum development be informed by patients, families and carers [1]. This has led to incorporation of patient perspectives into undergraduate healthcare professional (HCP) education. While the patient voice is increasingly prominent in rheumatology research, little has been published on its inclusion in rheumatology education, which appears to lag behind research.
Objectives: Recognising the importance of the patient voice, the British Society for Rheumatology (BSR) implemented a three-strand approach to embedding the patient voice across all educational outputs: 1) an in-person course co-designed with patients to showcase the patient voice, 2) a podcast series focused on patient perspectives, and 3) identifying patient partners to support BSR-led education.
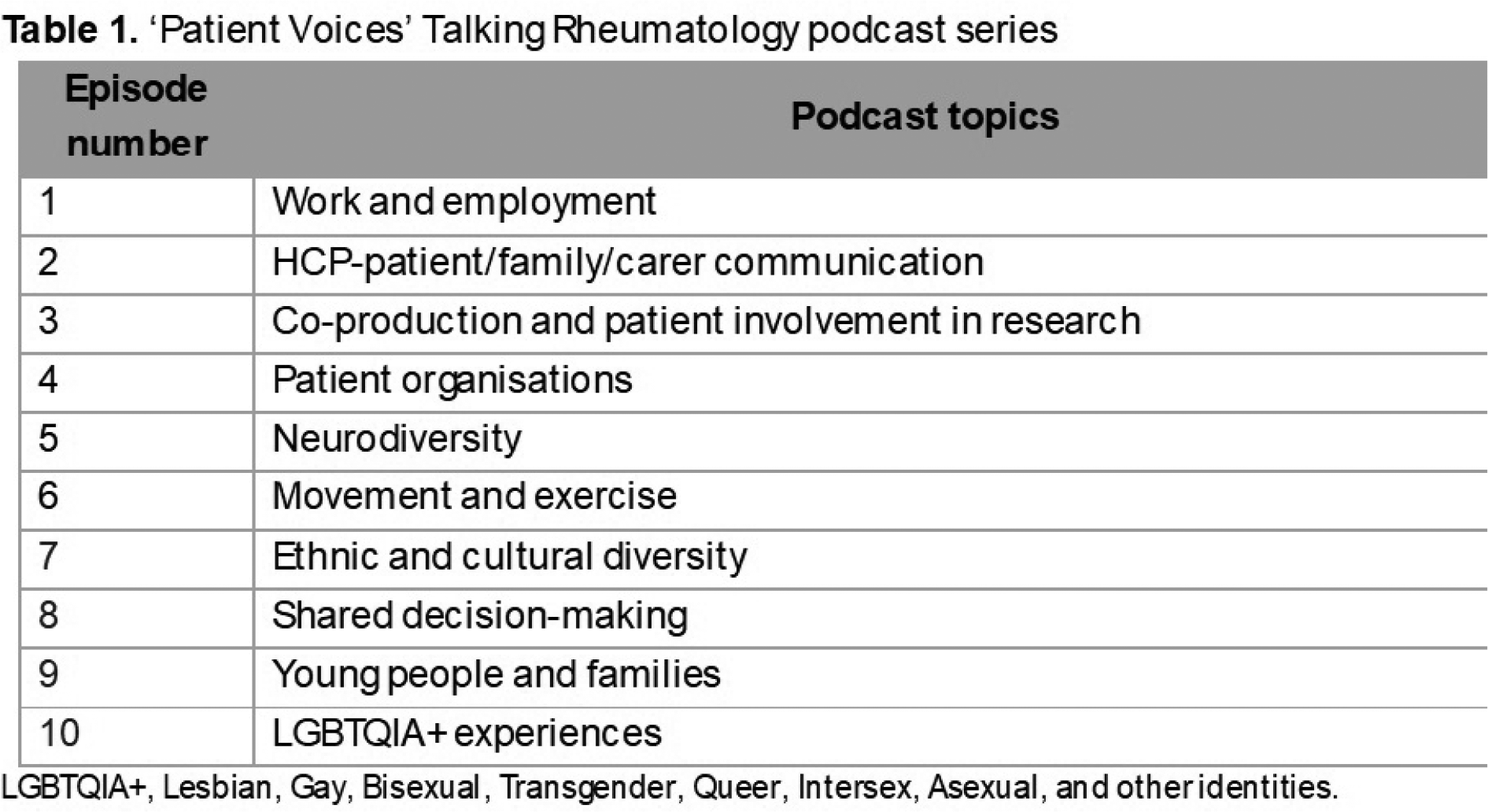
Methods: In June 2025, the inaugural ‘Patient Voices’ course was delivered in London. Patient experts were embedded in the faculty from inception, aligning with Towle Level 5 patient involvement [2]. The in-person course targeted HCPs working across the life course. Core themes included communication, supporting behaviour change and self-management, disability and diversity, and working with patient partners in service design and research. A blended educational approach, combining presentations and interviews delivered by patient experts, rheumatology HCPs and patient organisations. Participant numbers were capped to promote a relaxed environment and facilitate open discussion. Building on learning from this in-person course and BSR’s established digital reach, the patient voice was extended into digital education through a dedicated ‘Patient Voices’ Talking Rheumatology podcast series. The existing BSR Talking Rheumatology podcast (available on all podcasts platforms with over 100,000 downloads worldwide) demonstrated audience demand for patient-centred content, supported by over 1,070 downloads on a clinically focused episode co-delivered by a patient expert and rheumatologist. This informed commissioning of ten ‘Patient Voices’ episodes (Table 1). Patient experts were involved from the outset in shaping episode topics, guest communications, and podcast guidance. Invited podcast speakers include individuals with lived experience of rheumatic and musculoskeletal diseases (RMDs) and representatives from patient organisations, alongside other rheumatology topic experts. Pre-recording meetings were held to support confidence and clarify the scope of discussion. To further embed patient involvement across BSR education, an advertisement was developed to recruit patient partners to support ongoing and future BSR-led educational activities.
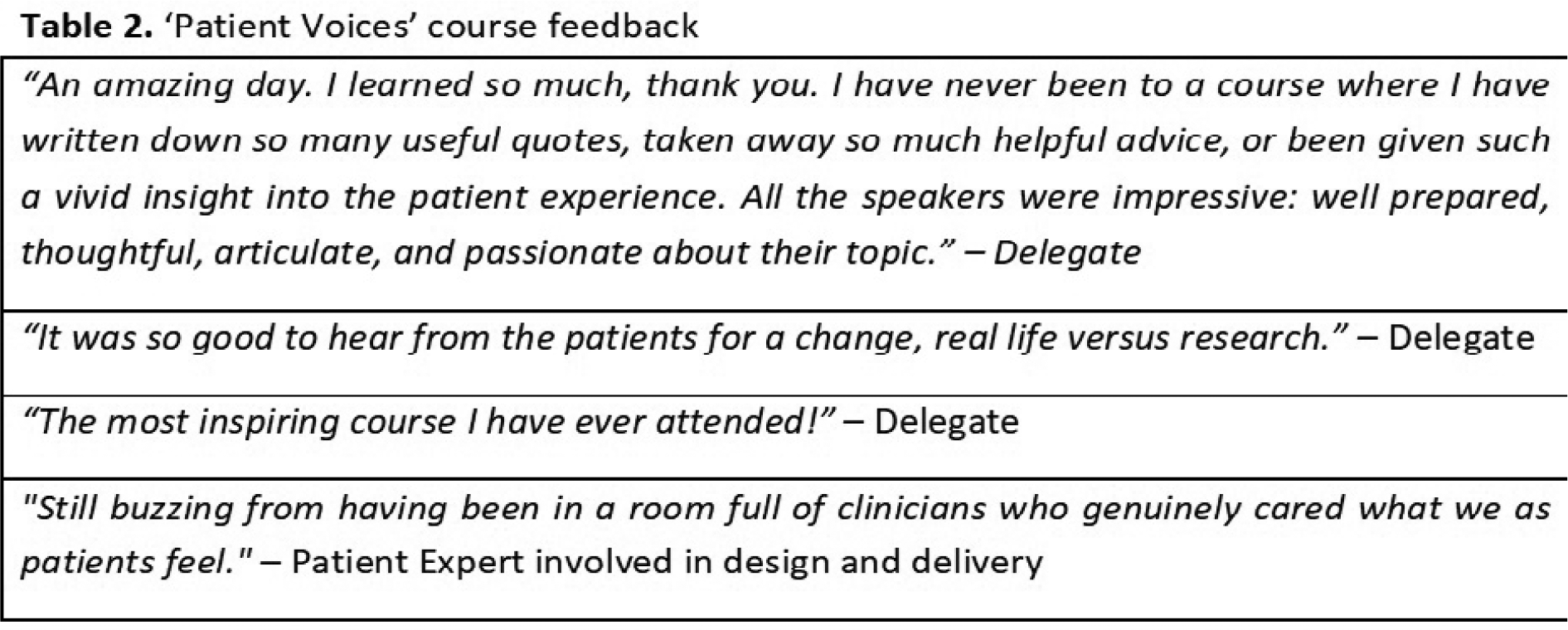
Results: The ‘Patient Voices’ course was attended by 70 delegates, including BSR staff, patient organisations, HCPs, patient experts and speakers. Feedback was collected via an online questionnaire (Table 2). All respondents (100%) reported that the learning objectives were met, 95% indicated the course would change their practice, and overall satisfaction was rated at 4.6/5. Course registration was initially slower than for other BSR education events. This was felt to reflect limited study leave for UK rheumatology HCPs and a perception that patient-centred topics may be a lower priority than clinically-focused education. However, attendee feedback demonstrated a strong perceived impact on practice, consist with Level 3 of Kirkpatrick’s evaluation model, indicating behaviour change following a high-level educational intervention (3). Building on the course, the ‘Patient Voices’ podcast series is scheduled to launch in April 2026. Evaluation is planned with patient partners and members of the BSR Education Committee, with episode-level feedback obtained via podcast platforms. Patient partners involved in the ‘Patient Voices’ course have already committed to further BSR educational projects. Identification of additional patient partners is underway through a digital advertisement to be shared widely, including via patient organisations.
Conclusions: This approach has provided a highly positive educational experience for both faculty, including HCPs and patient partners, and delegates. Feedback indicates high impact, with reported changes in practice that have the potential to improve patient care. These initiatives demonstrate the value of placing the patient voice at the centre of rheumatology education, with scope for wider adoption across the global rheumatology community.
REFERENCES: [1] General Medical Council (2011) Patient and Public involvement in undergraduate medical education. London: GMC.
[2] Towle A, Bainbridge L, Godolphin W, et al. Active patient involvement in the education of health professionals. Med Educ . 2010; 44 (1):64–.
[3] Kirkpatrick D. Great ideas revisited. Techniques for evaluating training programs. Revisiting Kirkpatrick’s four-level model. Train Dev . 1996; 50 :54–9.
Acknowledgments: NIL.
Disclosure of Interests: None declared.