fetching data ... 
Background: Implementing pharmacogenomics (PGx) in routine rheumatology practice is hindered by fragmented medication histories, EMR heterogeneity, and PGx reports that are often too technical for rapid clinical decision-making. A practical solution should (i) operate across different EMRs, (ii) support physician–patient communication with consent-respecting data sharing, and (iii) prioritize actionable variants relevant to a patient’s current medications.
Objectives: To describe a rheumatology-optimized PGx workflow that extends a polypharmacy-focused clinical decision support system (CDSS; InDream MediSupport) with patient-mediated data linkage via a PHR app (InDream MyChart), enabling real-time, actionable PGx alerts alongside multidimensional medication safety checks at the point of prescribing.
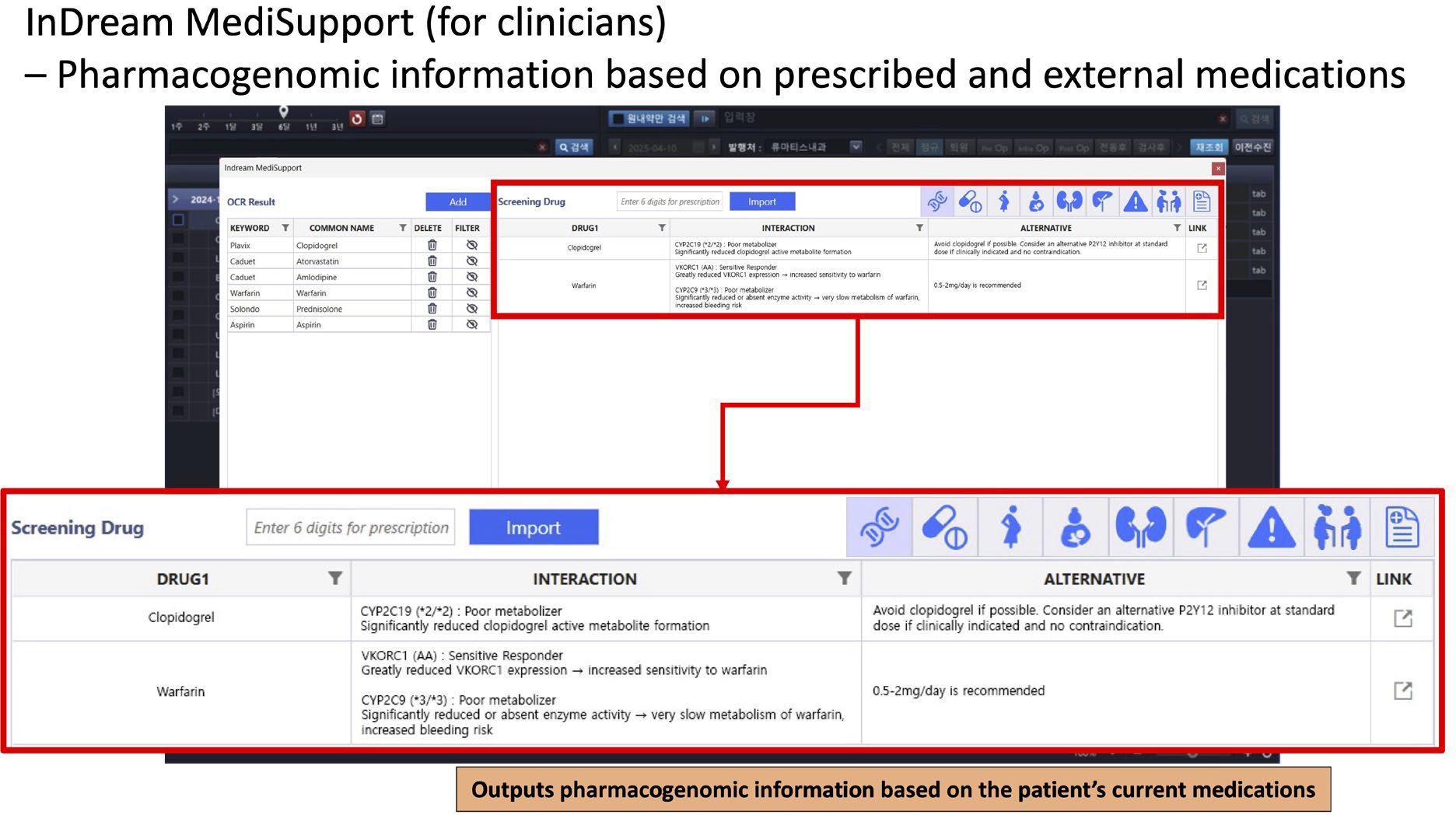
Methods: InDream MediSupport provides an EMR-agnostic architecture with two deployment modes: Type A (standalone, Smart Screen OCR) for rapid installation and immediate use, and Type B (EMR-integrated, standardized API) aligned with interoperability standards for seamless system integration. InDream MediSupport ( Baseline CDSS functions (non-PGx ) performs a 7-domain multidimensional safety check beyond conventional interaction alerts: (1) pharmacokinetic/pharmacodynamic drug–drug interactions, (2) pregnancy risk assessment based on regulatory categories, (3) lactation suitability and infant risk, (4) renal dose adjustment based on eGFR/CrCl, (5) hepatic impairment dosing using Child-Pugh/MELD, (6) potentially inappropriate medication screening for older adults using AGS Beers Criteria, and (7) detection of common and serious adverse reactions/allergy risks.
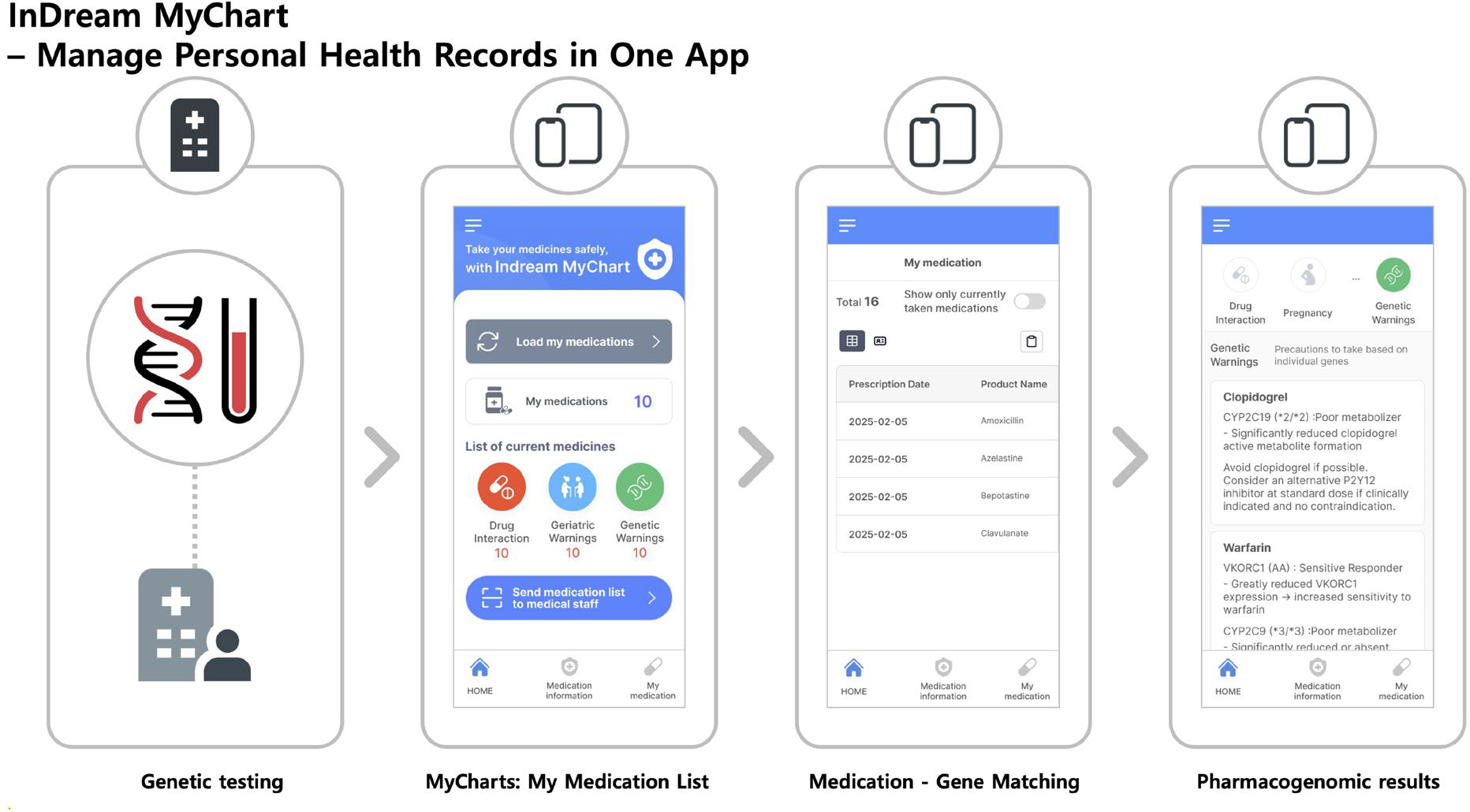
InDream MyChart (Patient-mediated data linkage) consolidates medication histories—including missing non-reimbursed or overseas prescriptions via OCR—and shares data to clinicians through a time-limited, one-time password (OTP)mechanism. When the clinician enters the OTP in MediSupport, outside prescriptions, allergy, and comorbidity data are loaded and cross-analyzed against intended prescriptions in real time, supporting a streamlined medication reconciliation process. The PGx module is built for practical use by focusing on (i) the patient’s current medications and (ii) genes with actionable variants, and by embedding curated guideline-based recommendations into the prescribing workflow. Key rheumatology-relevant gene–drug pairs included: azathioprine (TPMT/NUDT15) for myelosuppression risk, tacrolimus (CYP3A5) for initial dosing guidance, celecoxib/diclofenac (CYP2C9) for exposure/toxicity risk, and allopurinol (HLA-B*58:01) for severe cutaneous adverse reaction (SCAR) risk.
Results: The integrated system enables simultaneously applying multidimensional safety checks (interaction, pregnancy/lactation, renal/hepatic dosing, older-adult risks, and adverse event/allergy signals). In a user-experience survey of 12 physicians, mean checking time for a 10-drug regimen decreased from 8 minutes to 0.5 minutes for pregnancy/lactation safety and from 7 minutes to 0.5 minutes for renal dose adjustment when using InDream MediSupport (vs conventional references). Using conventional methods, the average time for drug–drug interaction checking was 11 minutes for 10 drugs. With MediSupport, completion times for pregnancy/lactation and renal-dose workflows were typically seconds to 1 minute (15 seconds 50.0%, 1 minute 25.0%, 5 seconds 16.7%, 3 minutes 8.3%). After adoption, use of existing drug-information websites/programs was unchanged in 50.0%, reduced by about half in 25.0%, and substantially reduced in 25.0%. If offered free of charge, 83.3% intended to continue using MediSupport after the beta period, 91.7% would recommend it to colleagues, and 91.6% agreed it was helpful for clinical care and/or patients. Overall satisfaction (5-point scale) was rated 3/5 by 58.3%, 4/5 by 33.3%, and 5/5 by 8.3%. Additionally, InDreamMyChart-to-InDreamMediSupport linkage was designed to reduce reliance on patient recall and shorten interview/medication-history acquisition time through rapid OTP-based loading and reconciliation support.
Conclusions: A rheumatology-optimized PGx workflow can be made clinically practical when embedded within an EMR-agnostic CDSS that already manages polypharmacy risks and is linked to a patient PHR app for consent-based data sharing. While comprehensive pharmacogenomic guidelines exist, limitations remain regarding clinical recommendations for some enzyme-drug interactions due to insufficient empirical evidence. Nevertheless, known enzyme substrates suggest extensive pharmacogenomic implications for numerous medications. Indream Healthcare’s pharmacogenomic database has cataloged hundreds of potential medication interactions, underscoring the broad applicability of genomic insights already achievable with existing patient genetic data. In conclusion, by coupling EMR-agnostic CDSS (InDream MediSupport) integration and patient-level genomic data via InDream MediChart, InDream Medisupport effectively bridges the gap between pharmacogenomic knowledge and clinical practice, potentially revolutionizing precision medication management.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Byeongzu Ghang Dr. Ghang is the founder and CEO of InDream Healthcare Inc., a company that develops digital health solutions, including a clinical decision support system for polypharmacy management., Dr. Ghang is the founder and CEO of InDream Healthcare Inc., a company that develops digital health solutions, including a clinical decision support system for polypharmacy management., Jay Chol Choi: None declared, Nayoung Han: None declared.