fetching data ... 
Background: In clinical practice, the majority of patients with psoriatic arthritis (PsA) present with mild-to-moderate skin involvement.[1] Interleukin-17 inhibitors (IL-17i) are generally favored for treating skin manifestations; however, there is limited real-world comparative evidence on standard-of-care treatments, such as tumor necrosis factor inhibitors (TNFi), and targeted synthetic treatments, such as upadacitinib (UPA), an oral Janus kinase inhibitor.
Objectives: The aim of this study was to compare the effectiveness of UPA, TNFi, and IL-17i therapies on skin symptoms in patients with PsA.
Methods: Data for this analysis were sourced from the Adelphi Real World Spondylarthritis (SpA) V and VI Disease Specific Programmes™, which are cross-sectional surveys. These surveys were conducted among physicians (rheumatologists, dermatologists, and internal medicine specialists) and their consulting patients during routine clinical practice. The studies spanned Germany, France, Italy, Spain, the United Kingdom (EU5; SpA V and VI), and the United States (US; SpA VI only). Data collection took place from March 2021 to November 2021 for SpA V, and from June 2023 to June 2024 for SpA VI. Adult patients with PsA who initiated treatment with either UPA, a TNFi, or an IL-17i were categorized into two groups for assessment: bio-naïve (EU5) and those with prior TNFi exposure (EU5 and US). Physician-reported outcomes on the presence or absence (yes/no) of psoriatic skin lesions, genital psoriasis, scalp psoriasis, nail deformation, and mild-to-no skin involvement were evaluated at least 3 months after treatment initiation. Patient demographics and disease-related characteristics were adjusted using an entropy balancing approach, adjusted for age, sex, disease severity, skin severity, psoriatic skin lesions, genital psoriasis, scalp psoriasis, and nail deformation at initiation of treatment. Entropy-balanced analyses were performed separately for comparisons between UPA vs TNFi and between UPA vs IL-17i.
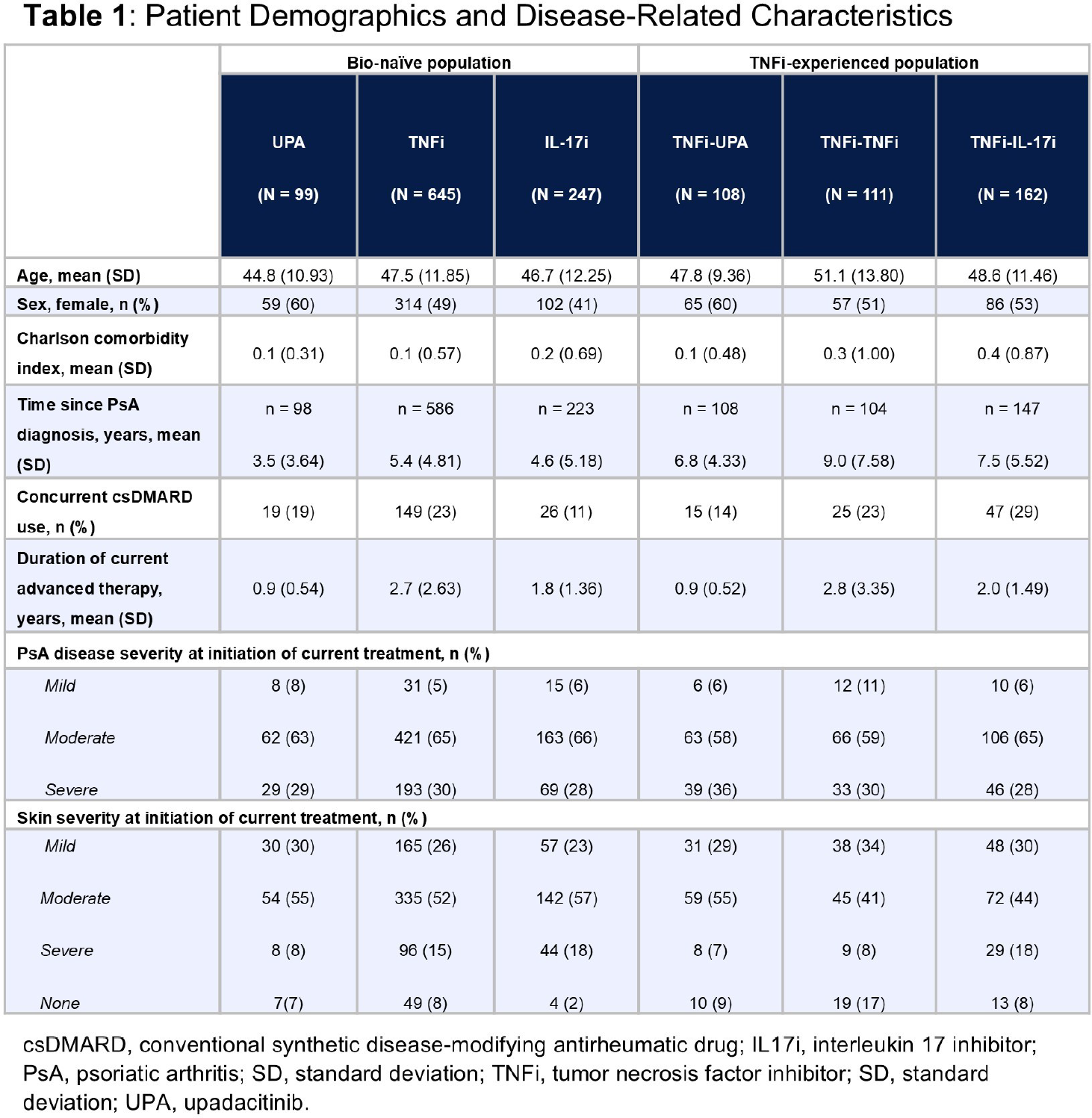
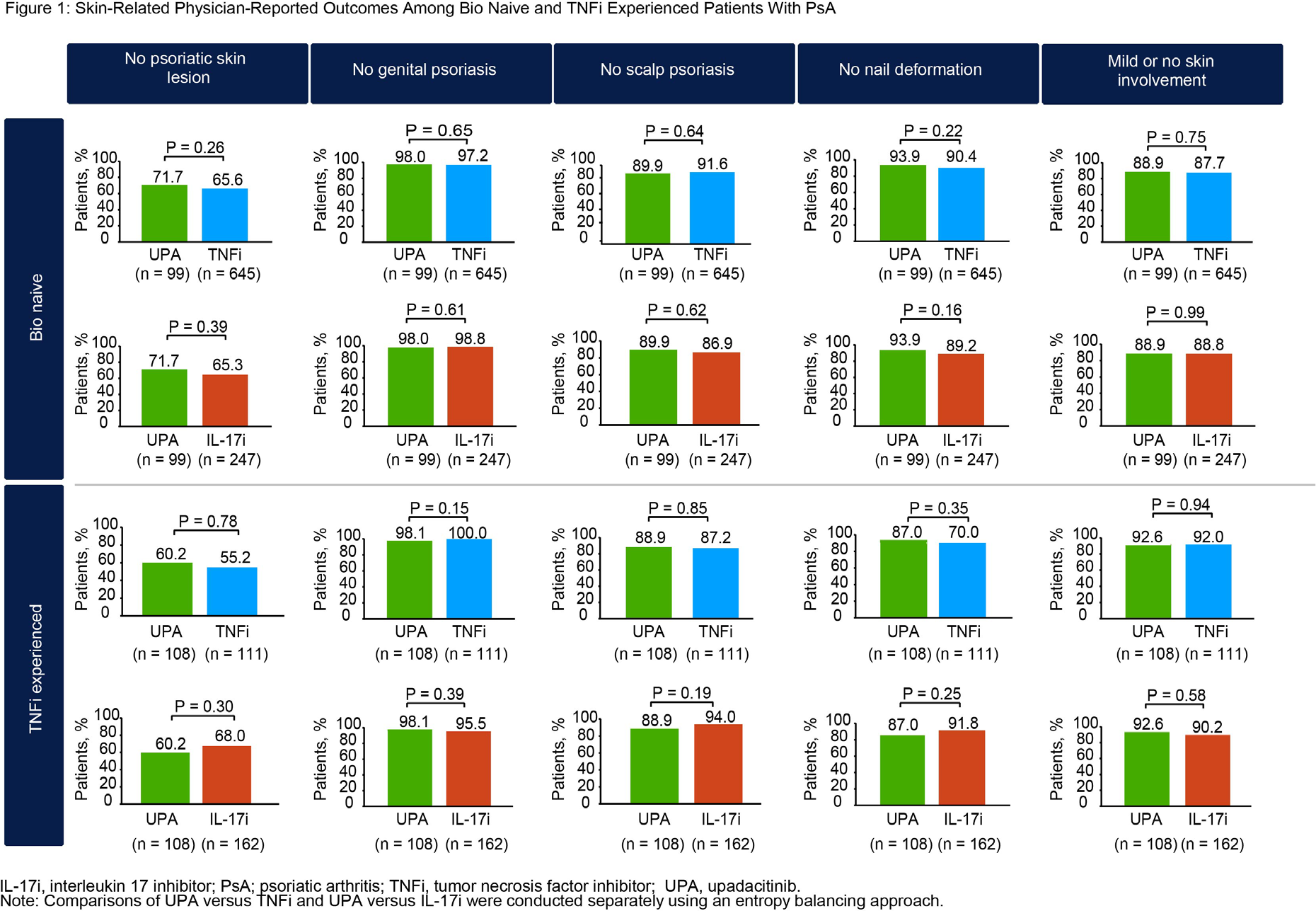
Results: Among the 991 patients who were bio-naïve, 99 initiated UPA, 645 initiated a TNFi, and 247 initiated an IL-17i. Of the 381 patients who had prior exposure to TNFi, 108 initiated UPA, 111 initiated another TNFi, and 162 initiated an IL-17i. Patient demographics are detailed in Table 1 . Adalimumab was the most frequently used TNFi, while secukinumab was the most commonly used IL-17i. Across groups, most patients (approximately 74-85%) had mild-to-moderate skin severity at the time of treatment initiation. The mean duration of current advanced therapy in the bio-naïve population was 0.9 years for UPA, 2.7 years for TNFi, and 1.8 years for IL-17i. After adjusting for covariates using entropy balancing, physician-reported outcomes for the bio-naïve population in the UPA group were comparable to those in the TNFi group (no psoriatic skin lesions: 71.7% vs 65.6%; P = 0.26; no genital psoriasis: 98.0% vs 97.2%; P = 0.65; no scalp psoriasis: 89.9% vs 91.6%; P = 0.64; no nail deformation: 93.9% vs 90.4%; P = 0.22 and mild to no skin involvement: 88.9% vs 87.7%; P = 0.75) and in the IL-17i group (71.7% vs 65.3%; P = 0.39; 98.0% vs 98.8%; P = 0.61; 89.9% vs 86.9%; P = 0.62; 93.9% vs 89.2%; P = 0.16 and 88.9% vs 88.8%; P = 0.99) at the time of data collection ( Figure 1 ). Comparable results were observed in patients with prior exposure to TNFi, with no significant difference in the proportions of patients achieving the outcomes in the UPA group versus those in the TNFi group (60.2% vs 55.2%; P = 0.78; 98.1% vs 100.0%; P = 0.15; 88.9% vs 87.2%; P = 0.85; 87.0% vs 70.0%; P = 0.35 and 92.6% vs 92.0%; P = 0.94) or the IL-17i group (60.2% vs 68.0%; P = 0.30; 98.1% vs 95.5%; P = 0.39; 88.9% vs 94.0%; P = 0.19; 87.0% vs 91.8%; P = 0.25 and 92.6% vs 90.2%; P = 0.58) ( Figure 1 ).
Conclusions: In this real-world study, over three-quarters of patients with PsA presented with mild-to-moderate skin severity at treatment initiation. Patients who were prescribed with UPA showed comparable presence of skin symptoms versus those who initiated a TNFi or an IL-17i, regardless of prior TNFi treatment status.
REFERENCES: [1] Mease PJ et al. J Rheumatol . 2017; 44(8):1151-58.
Acknowledgments: NIL.
Disclosure of Interests: Philip J. Mease has received consultancy fees or honoraria from AbbVie, Acelyrin, Amgen, BMS, Century, Cullinan Biotech, Eli Lilly, Inmagene, Johnson & Johnson, MoonLake Immunotherapeutics AG, Novartis, Pfizer, Takeda, UCB, has participated on a safety monitoring board at Genascence and holds a leadership or fiduciary role at GRAPPA, OMERACT, and SpartAN, grants or contracts from AbbVie, Amgen, Acelyrin, BMS, Eli Lilly, Johnson & Johnson, Novartis, Pfizer, and UCB, William Tillett has received speaker fees from AbbVie, Amgen, BMS, Celgene, Eli Lilly, GSK, Janssen, MSD, Novartis, Ono, Pfizer, UCB, consulting fees from AbbVie, Amgen, BMS, Celgene, Eli Lilly, GSK, Janssen, MSD, Novartis, Ono, Pfizer, UCB, research grants from AbbVie, Amgen, Eli Lilly, Janssen, Pfizer, UCB, Xiaolan Ye may hold stock or stock options at AbbVie, employee of AbbVie, Christopher D Saffore may hold stock or stock options at AbbVie, employee of AbbVie, Molly Edwards employee of Adelphi Real World, acted as a consultant to AbbVie, Isabel Truman employee of Adelphi Real World, acted as a consultant to AbbVie, Gary Milligan employee of Adelphi Real World, acted as a consultant to AbbVie, AVANI Joshi may hold stock or stock options at AbbVie, employee of AbbVie, Bhumik Parikh may hold stock or stock options at AbbVie, employee of AbbVie, Lucia Novelli may hold stock or stock options at AbbVie, employee of AbbVie, Daniel Aletaha received speakers’ bureau fees from AbbVie, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer, Sandoz and Sanofi, consulting fees or honoraria from AbbVie, Amgen, BMS, Biogen, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer, Sandoz, Sanofi, UCB, and Viatris, received grant/research support from AbbVie, Biogen, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer, Sandoz, Sanofi, and UCB.