fetching data ... 
Background: With population ageing, frailty is becoming increasingly prevalent in daily rheumatology practice. Assessing frailty in rheumatoid arthritis (RA) is challenging, partly because consequences of RA may overlap with manifestations of frailty. Two widely used frailty instruments in the general older population are the Groningen Frailty Indicator (GFI) and Fried frailty criteria. The GFI is a biopsychosocial multidimensional self-report questionnaire, while the Fried criteria represent an observer-assessed physical frailty phenotype. Despite the potential value of frailty assessment in RA, it is unknown whether and how frailty instruments compare between older adults with RA and population controls, and whether ageing is accelerated in RA.
Objectives: This study aims to compare for each instrument (1) the prevalence of (pre)frailty between RA and controls, and (2) factors driving (pre)frailty in RA compared to controls.
Methods: Cross-sectional data from the STudying Ageing in Rheumatoid arthritis (STAR) study were used, including patients with RA and population controls without inflammatory rheumatic disease aged 55–85 years. Frailty was assessed using the GFI (15 items (yes/no); physical, cognitive, social, and psychological domains; frail=score≥4/15 [1]) in all participants and the Fried criteria (5 domains; weight loss, exhaustion, low physical activity, slow gait, low grip strength; frail=≥3 deficits, prefrail=1-2 deficits [2]) in a subgroup who additionally underwent a clinical assessment. Prevalence of (pre)frailty is described by group (RA/control). Next, uni- and multivariable logistic (GFI; frail vs. robust) and Poisson (Fried; (pre)frail vs. robust) regressions assessed whether the association between age and (pre)frailty differs between RA and controls (interaction age*group) and explored the role of additional confounders and covariates (sociodemographic (e.g. sex, marital status), lifestyle (e.g. smoking status, body mass index (BMI)), and clinical factors (e.g. comorbidities (Charlson Comorbidity Index (CCI)), fatigue (Multidimensional Fatigue Inventory (MFI)), physical function (Health Assessment Questionnaire-Disability Index (HAQ-DI)), anxiety (Generalized Anxiety Disorder-7 (GAD-7)).
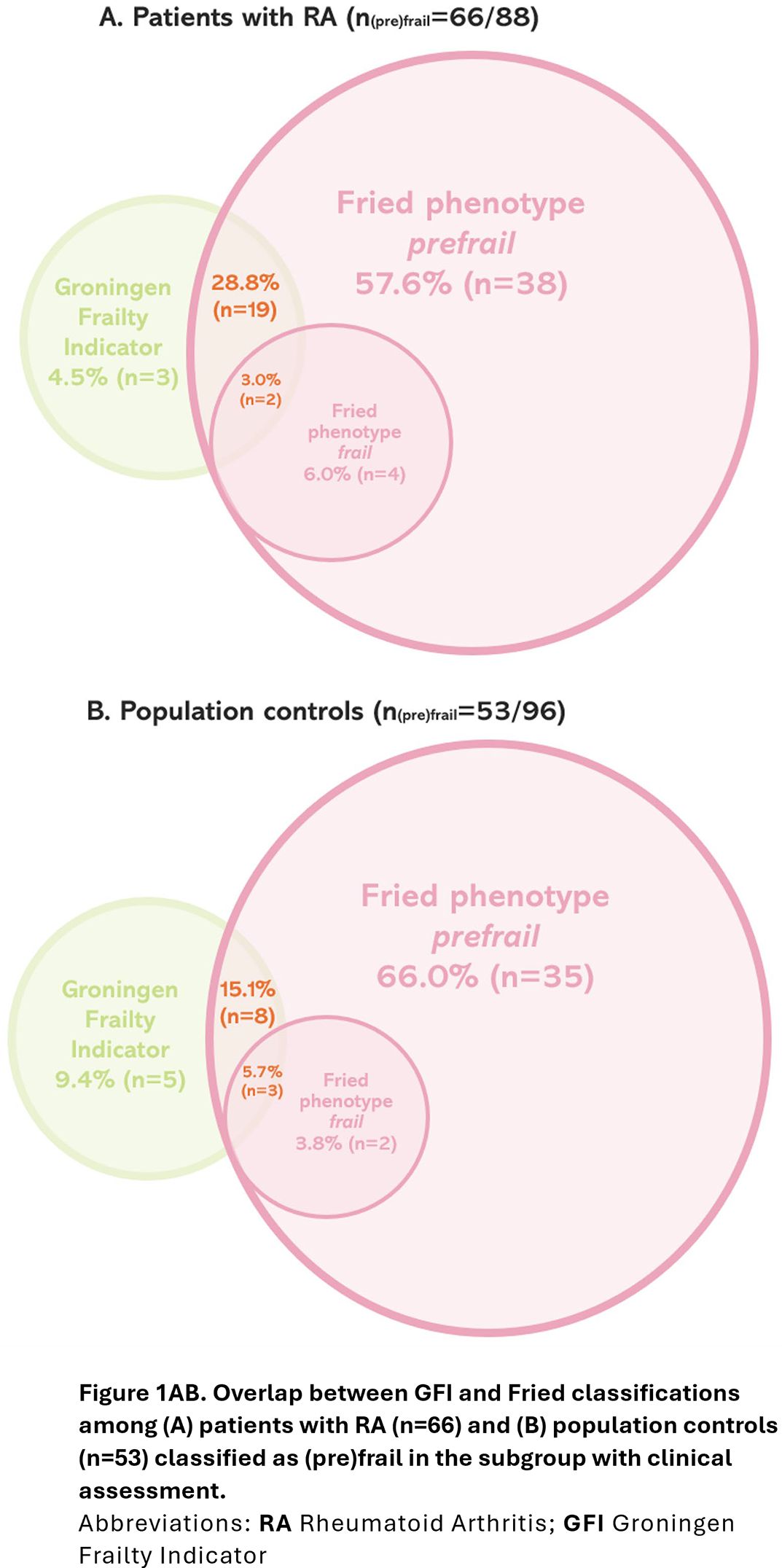
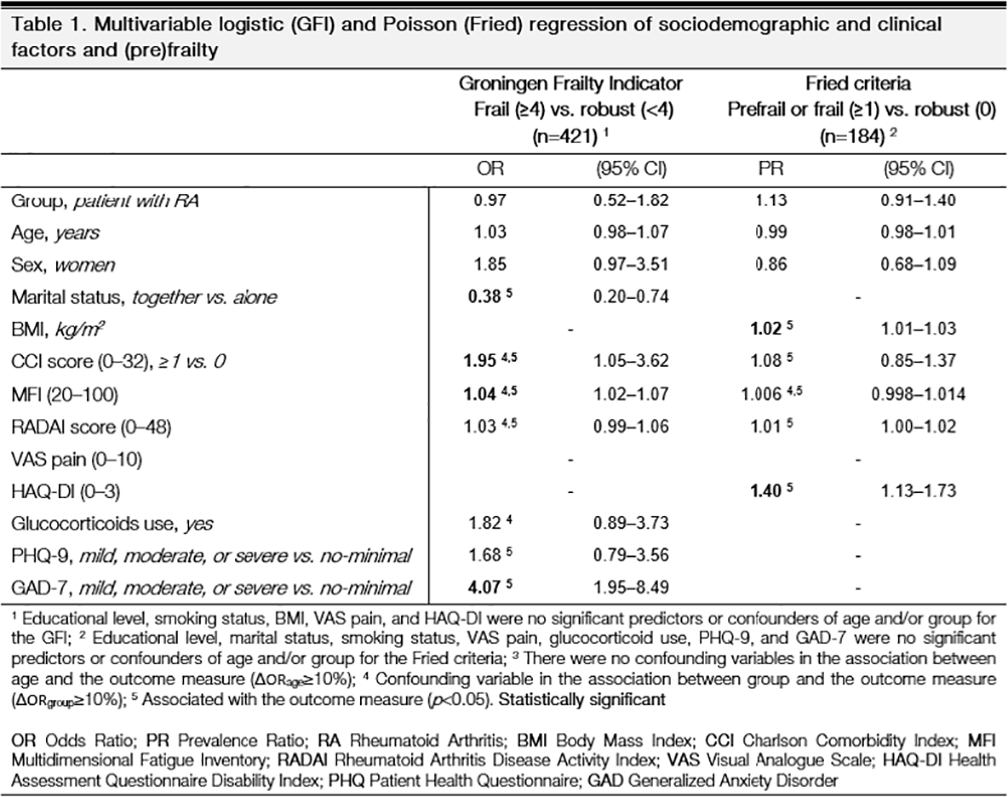
Results: A total of 421 participants were included: 207 patients with RA (mean age 68 (SD 7); 62% women) and 214 population controls (mean age 68 (7); 60% women). The subgroup with clinical assessment comprised 196 participants: 88 patients with RA (mean age 67 (8); 51% women) and 96 controls (mean age 68 (8); 55% women). A higher proportion of patients with RA than controls was classified as (pre)frail by the GFI (RA: 34% (n=70/207) vs. controls: 18% (n=38/214)) as well as Fried criteria (Fried pre-frail: RA: 65% (n=57/88) vs. controls: 50% (n=48/96); Fried frail: RA: 7% (n=6/88) vs. controls: 5% (n=5/96)). Of note, 88% (n=21/24) of patients with RA classified as frail by the GFI were also (pre)frail by the Fried criteria, while less overlap was observed in controls (69% (n=11/16)) (Figure 1AB). Age was not associated with (pre)frailty in uni- or multivariable analyses for either instrument, in RA nor controls ( p interaction age*group >0.10) (Table 1). RA was associated with (pre)frailty as defined by both the GFI (OR=2.4, 95%CI: 1.5–3.8) and Fried criteria (PR=1.4, 95%CI: 1.1–1.8) in univariable analyses, but these associations were no longer observed after multivariable adjustment. In the final models, other factors associated with GFI-defined frailty included living alone, a comorbidity score ≥1, higher fatigue (MFI), and mild to severe anxiety. Factors associated with Fried (pre)frailty were a higher BMI and especially poorer physical function (HAQ-DI).
Conclusions: (Pre)frailty was more common in older adults with RA than in population controls. The Fried criteria - focusing on the detection of a physical frailty phenotype - classified more patients with RA than controls as (pre)frail compared to the GFI. However, this is explained completely by the physical consequences of RA. The GFI discriminates somewhat less between RA and population controls and more strongly reflects social and psychological vulnerability. Together with the lack of an association between frailty and age, it can be questioned whether current frailty instruments are useful to detect the negative consequences of ageing beyond the impact of RA itself.
REFERENCES: [1] Fried, L. P., et al. (2001). Frailty in older adults: evidence for a phenotype. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences , 56 (3), M146-M157.
[2] Steverink, N. et al. (2001). Measuring frailty: developing and testing the GFI (Groningen Frailty Indicator). The gerontologist , 41 , 236.
Acknowledgments: NIL.
Disclosure of Interests: Saskia Truijen: None declared, Annelies Boonen AbbVie, Celgene, UCB, Eli Lilly, Novartis, Sandoz, Alfasigma, Sofia Ramiro AbbVie, Alfasigma, Eli Lilly, MSD, Novartis, Pfizer, Takeda, UCB, AbbVie, Alfasigma, Eli Lilly, MSD, Novartis, Pfizer, Takeda, UCB, Marloes van Onna Novartis, Pfizer, Alfasigma, Pfizer, ReumaNederland.