fetching data ... 
Background: Tapering biological disease-modifying anti-rheumatic drugs (bDMARDs) in rheumatoid arthritis (RA) aims to reduce drug exposure, adverse effects and costs while maintaining disease control, but is associated with increased flare risk. No baseline variables predict flare risk with sufficient accuracy during bDMARD tapering [1]. Previously, a dynamic multivariate prediction model was developed and validated to repeatedly estimate 3-monthly flare risk at each disease activity-guided tapering step, enabling guidance for further tapering decisions [2]. This has the potential to reduce flares and still preserve optimal dose reduction.
Objectives: To evaluate whether prediction-aided bDMARD tapering (PAT) reduces the occurrence of flares compared with disease activity–guided stepwise tapering (DGT).
Methods: PATIO was a pragmatic, multicentre, open-label, randomised controlled superiority trial including 162 RA patients with sustained low disease activity on bDMARD therapy. Patients were randomised 1:1 to DGT or DGT combined with a criterion based on predicted flare risk, prediction-aided tapering (PAT) and followed up for 18 months. The primary outcome was the number of flares per patient, analysed using negative binomial regression with follow-up time as offset and adjustment for baseline DAS28, bDMARD line, csDMARD use, and study site. Flares were defined as an increase in DAS28 of 1.2 points from baseline or an increase of 0.6 points with a current DAS28 >2.9. Predefined per-protocol (PP) populations reflected adherence to tapering advice and stability of csDMARD treatment. Secondary outcomes included the occurrence of any flare or major flare (flare duration >12 weeks), DAS28-CRP over time, mean bDMARD dose (fraction of maximum dose), infections requiring antibiotics, and patient-reported outcomes (HAQ, EQ-5D).
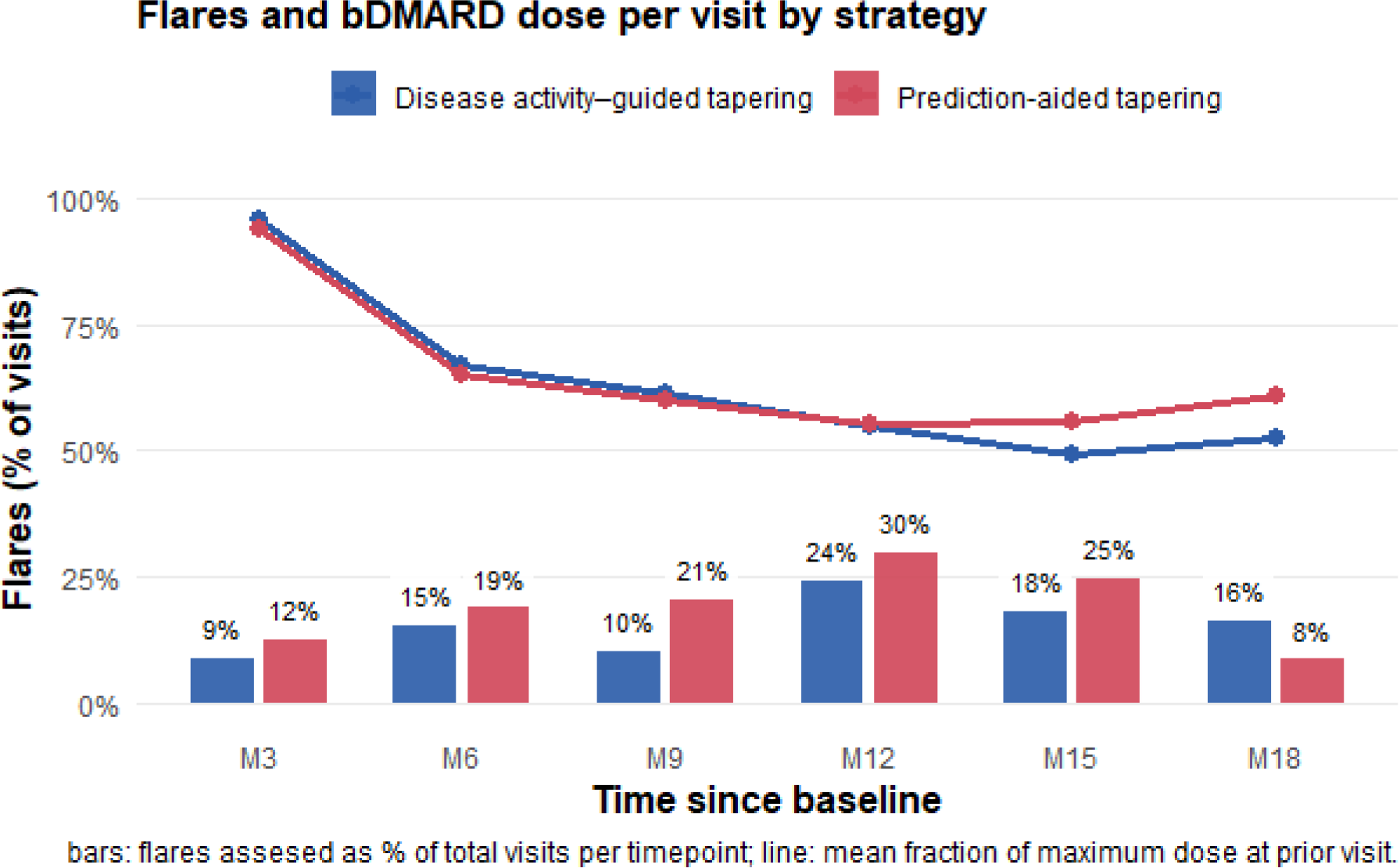
Results: A total of 162 patients were recruited and included in the ITT analysis, with 81 patients randomized to both DGT and PAT. Non-adherence to tapering advice occurred frequently, at least once in 46% and 58% of patients in PAT/DGT. Ignoring advice to continue tapering was more frequent in DGT (44% vs 25%), whereas ignoring advice to stop tapering occurred more often in PAT (17% vs 11%). Over 18 months, the mean number of flares per patient was 1.06 (95% CI 0.80–1.33) in the PAT group and 0.83 (95% CI 0.60–1.05) in the DGT group. The rate ratio (RR) was 1.26 (95% CI 0.89–1.79) in favour of DGT ( Figure 1 ). Per protocol analyses confirmed the ITT analysis, with results indicating no difference or a non-statistically significant higher flare risk in PAT, with RR between 1.21 (95% CI 0.79–1.87) and 1.61 (95% CI 0.84–3.18). Any flare occurring was observed in 56% of patients (PAT) and 51% in DGT (adjusted OR 1.22, 95% CI 0.62–2.37). Major flares happened in 23% of PAT and 12% of DGT patients (adjusted OR 2.39, 95% CI 0.95–6.00). DAS28-CRP trajectories were similar between the groups (mean DAS28 of 2.2 in PAT vs 2.1 in DGT, mean difference 0.09, 95% CI −0.13 to 0.31) with no significant differences over time (p=0.853). The mean bDMARD dose fraction was 0.57 for DGT and 0.59 for PAT (mean difference 0.02, 95% CI −0.05 to 0.09). No differences were observed in patient-reported outcomes, with a mean HAQ of 0.75 in DGT and 0.77 in PAT (mean difference 0.02, 95% CI −0.07 to 0.11), and a mean EQ-5D of 0.83 in DGT and 0.82 in PAT (mean difference -0.02, 95% CI -0.06 to 0.01). Infection rates were comparable between strategies (adjusted OR 0.73, 95% CI 0.36–1.50).
Conclusions: In this pragmatic randomized trial, prediction-aided tapering did not reduce flare rates compared with disease activity–guided tapering in patients with rheumatoid arthritis receiving stable bDMARD therapy. Outcomes in the control arm were consistent with those of previous stepwise tapering trials, confirming the effectiveness of disease activity–guided tapering alone. High non-adherence and differences in adherence patterns between groups indicate that the prediction tool influenced tapering behaviour rather than improving clinical outcomes. These findings suggest that prediction-aided tapering should not be implemented in routine clinical practice at this time.
| Variable | DGT | PAT |
|---|---|---|
| n | 81 | 81 |
| Age (years) (median [IQR] ) | 61[52, 69] | 61 [52, 67] |
| DAS28 (mean (SD )) | 1.9 (0.6) | 1.9 (0.6) |
| Tender joint count (28) (median [IQR] ) | 0.0 [0.0, 1.0] | 0.0 [0.0, 1.0] |
| Swollen joint count (28) (median [IQR] ) | 0.0 [0.0, 0.0] | 0.0 [0.0, 0.0] |
| CRP (mg/L) (median [IQR] ) | 1 [0.5, 3.0] | 1 [0.5, 2.0] |
| Body Mass Index (kg/m 2 ) (mean (SD ) | 27 (6.0) | 27 (4.7) |
| Years since diagnosis (median [IQR] ) | 6.0 [2.0, 12.0] | 7.0 [2.0, 15.0] |
| Biological dose at baseline (fraction of max dose, SD ) | 0.96 (0.11) | 0.94 (0.13) |
| HAQ at baseline (mean (SD )) | 0.64 (0.59) | 0.60 (0.60) |
| EQ-5D VAS at baseline (mean (SD )) | 73 (21) | 70 (22) |
| EQ-5D index (NL) at baseline (mean (SD )) | 0.83 (0.16) | 0.84 (0.11) |
| ACPA (positive) (% ) | 48 (60.0) | 45 (57.0) |
| Rheumatoid factor (positive)% ) | 44 (56.4) | 42 (53.8) |
| Sex (female) (% ) | 55 (67.9) | 51 (63.0) |
| Biological type = Non-TNF (% ) | 16 (19.8) | 16 (19.8) |
| csDMARD use at baseline (% ) | 65 (80.2) | 63 (77.8) |
| Methotrexate use at baseline (% ) | 45 (55.6) | 55 (67.9) |
REFERENCES: [1] Tweehuysen L, van den Ende CH, Beeren FM, Been EM, van den Hoogen FH, den Broeder AA. Little Evidence for Usefulness of Biomarkers for Predicting Successful Dose Reduction or Discontinuation of a Biologic Agent in Rheumatoid Arthritis: A Systematic Review. Arthritis Rheumatol. 2017;69(2):301-8.
[2] van der Leeuw MS, Messelink MA, Tekstra J, Medina O, van Laar JM, Haitjema S, et al. Using real-world data to dynamically predict flares during tapering of biological DMARDs in rheumatoid arthritis: development, validation, and potential impact of prediction-aided decisions. Arthritis Research & Therapy. 2022;24(1):74.
Acknowledgments: NIL.
Disclosure of Interests: Sina Fadaei: None declared, A.A. den Broeder: None declared, Amin Herman: None declared, Harald E. Vonkeman HEV has received research grants from Galapagos and Boehringer Ingelheim, and consulting fees from AbbVie, Novartis, Pfizer, UCB, Alphasigma, and Johnson and Johnson, all outside the current work., Judith Peeters: None declared, Annelies Maas: None declared, Julia Spierings: None declared, Jacob M. van Laar JMvL received honoraria from Abbvie, Alfasigma, Alentis, Amgen, Astra Zeneca, Boehringer Ingelheim, Eli Lilly, GSK, Novartis, JMvL received research grants from Alfasigma and Boehringer Ingelheim., Janneke Tekstra: None declared, Marianne A. Messelink: None declared, Pauline Bovens: None declared, Marlies van der Goes: None declared, Paco Welsing: None declared.