fetching data ... 
Background: Improved life expectancy and advances in treatment have resulted in a growing population of older patients with rheumatoid arthritis (RA). However, evidence on the comparative safety of different disease-modifying antirheumatic drug (DMARD) classes in this age group remains limited. Serious infections (SI) are a major concern with immunosuppressive therapies, particularly in older adults who may have increased baseline risk due to comorbidities and age-related immune changes. ([1,2]).
Objectives: To compare the occurrence of SI among older adults with RA receiving different DMARD classes (conventional synthetic (cs), biologics (b): TNFi, IL6i, B-cell-targeted, T-cell-modulating, and targeted synthetics (ts): JAKi) in a real-world setting.
Methods: Data were used from the German DMARD register RABBIT (Rheumatoid Arthritis: Observation of Biologic Therapy). All treatment episodes from patients initiating DMARD therapy after January 1, 2017, were identified to obtain comparable enrollment periods for all DMARDs upon the first JAKi availability in Germany. Patients could contribute multiple treatment episodes; standard errors were computed using patient-clustered robust (sandwich) estimators. Two complementary analyses were conducted. First, to assess age-dependent risks of SI (hazard ratio, HR) in the RABBIT cohort, we used spline functions to model the effect of age in Cox proportional hazards models (CPH) including all RA patients. Second, to evaluate DMARD-specific effects in older patients, analyses were restricted to patients aged ≥ 60 years. Treatment groups were adjusted for confounding using weighting methods. Identified confounders included age, sex, BMI, glucocorticoid dosage, disease activity (DAS28), functional status (Hannover Functional Questionnaire, FFbH), disease duration, prior DMARD exposure, smoking history, and comorbidities (diabetes, pulmonary fibrosis, COPD, renal disease, malignancy). Inverse probability of censoring weighting was used to adjust for selective dropout, and multiple imputation was applied for missing data using 20 imputations.
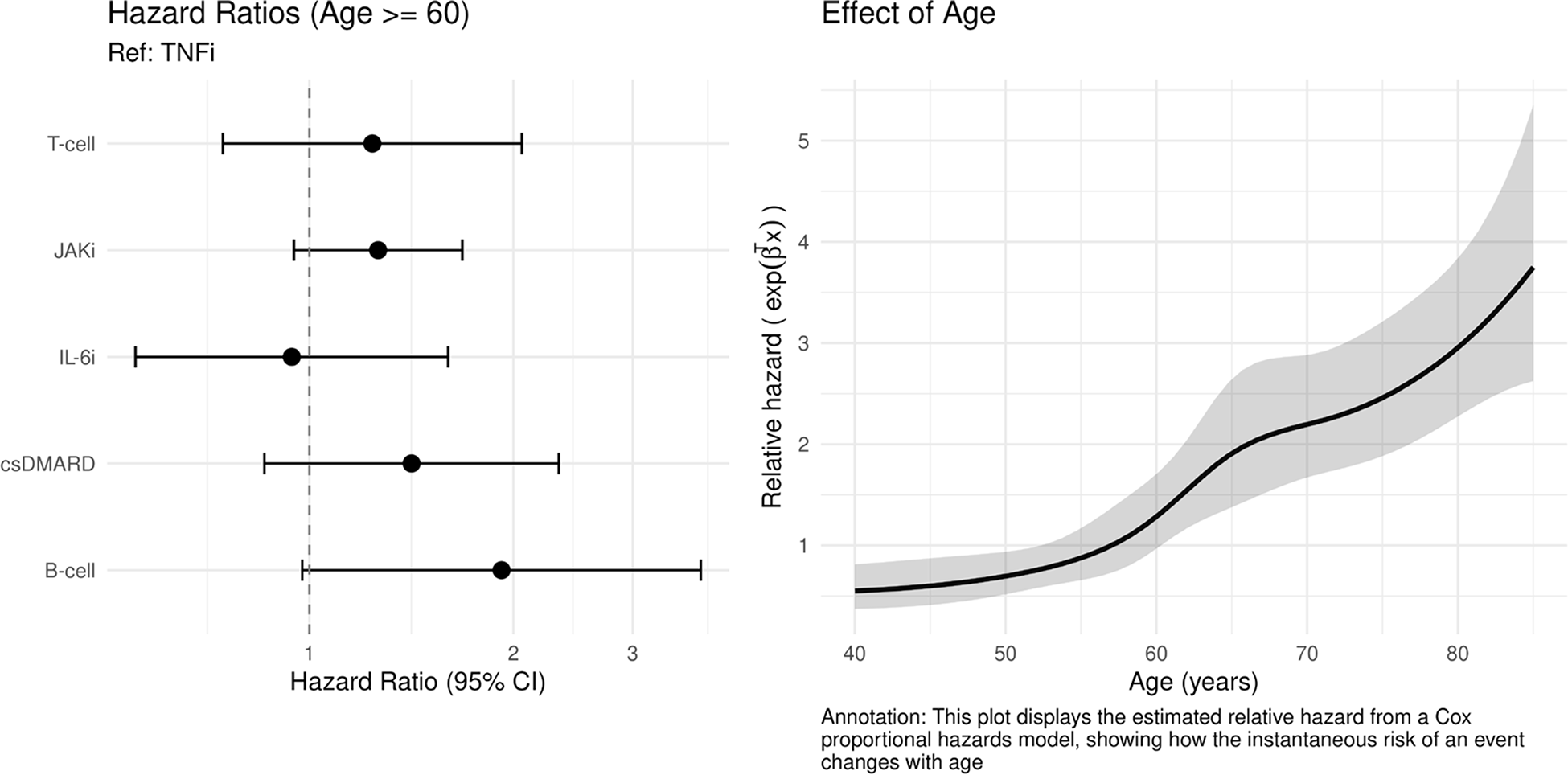
Results: The CPH model using spline functions to model age-dependent risks of SI included 10375 patients contributing 21019 episodes and shows an increasing relative hazard ( Figure 1 , right), demonstrating substantial age-related vulnerability. For the second analysis, a total of 11213 treatment episodes from 5684 patients aged ≥60 years initiating six different DMARD classes were included. Baseline characteristics were already balanced across treatment groups prior to weighting, e.g., comparable disease activity was observed across b/ts DMARD classes. However, prior disease duration and the number of prior b/ts DMARDs varied notably by treatment group ( Table 1 ). These differences were attenuated after weighting for confounding factors. Compared to TNFi, HRs for SI are shown in Figure 1 (left). IL6i therapy showed comparable risk to TNFi. T-cell, JAKi, csDMARD, and B-cell treatments showed numerically higher risk estimates, that were not statistically significant.
Conclusions: Among older RA patients, IL6i were associated with a risk of SI comparable to TNFi, while other DMARD classes showed non-significantly increased risk estimates. The age-dependent risk of SI suggests that chronological age (and associated comorbidities) may outweigh treatment-specific factors when assessing vulnerability to infection. This study underscores the importance of infection vigilance in this population, irrespective of the immunosuppressive agent chosen.
Hazard ratios for DMARD therapies versus TNFi in patients aged≥60 years (left) and effect of age on relative hazard (right).
Baseline characteristics for older adults (age≥60)
| DMARD classes | TNFi | B-cell | T-cell | IL6i | JAKi | csDMARD |
|---|---|---|---|---|---|---|
| No. episodes | 3,209 | 1,048 | 733 | 1,089 | 2,417 | 2,717 |
| Sex, n (%) | ||||||
| Male | 881 (27.5%) | 316 (30.2%) | 201 (27.4%) | 306 (28.1%) | 561 (23.2%) | 762 (28.0%) |
| Female | 2,328 (72.5%) | 732 (69.8%) | 532 (72.6%) | 783 (71.9%) | 1,856 (76.8%) | 1,955 (72.0%) |
| Age [years], Mean (SD) | 69.7 (7.0) | 70.1
| 70.4 (7.1) | 69.1 (7.0) | 69.5 (7.0) | 70.2
|
| Disease activity [DAS28], Mean (SD) | 4.4 (1.4) | 3.6 (1.4) | 4.3 (1.4) | 4.4 (1.5) | 4.4 (1.4) | 3.8 (1.3) |
| Functional capacity [FFbH, % of full function], Mean (SD) | 63.5 (23.8) | 63.6 (24.1) | 59.4 (24.3) | 60.9 (24.8) | 60.9 (24.5) | 64.3
|
| RA disease duration [years],
| 11.3 (10.1) | 17.2 (10.3) | 13.6 (10.6) | 12.8 (10.4) | 13.6 (10.2) | 13.0
|
| Glucocorticoid dose [mg/day] in the last 6 months, Mean (SD) | 3.5 (4.8) | 2.6 (3.9) | 3.4 (4.7) | 3.5 (5.1) | 3.3 (4.2) | 2.8 (4.2) |
| Number of prior b/ts DMARDs, Mean (SD) | 1.4 (0.9) | 2.5 (1.0) | 2.3 (1.1) | 2.2 (1.0) | 1.5 (1.3) | 0.7 (1.1) |
| Number of prior csDMARDs, Mean (SD) | 1.6 (0.5) | 1.8 (0.4) | 1.7 (0.5) | 1.6 (0.5) | 1.6 (0.5) | 2.0 (0.2) |
| Diabetes, n (%) | 555 (17.3%) | 187 (17.8%) | 152 (20.7%) | 215 (19.7%) | 458 (18.9%) | 488
|
| COPD, n (%) | 257 (8.0%) | 140 (13.4%) | 107 (14.6%) | 105 (9.6%) | 224 (9.3%) | 292
|
| Pulmonary fibrosis, n (%) | 37 (1.2%) | 42
| 60 (8.2%) | 18 (1.7%) | 49 (2.0%) | 67
|
| Kidney disease, n (%) | 377 (11.7%) | 111 (10.6%) | 109 (14.9%) | 139 (12.8%) | 314 (13.0%) | 250
|
| Malignancy, n (%) | 260 (8.1%) | 157 (15.0%) | 93 (12.7%) | 86 (7.9%) | 180 (7.4%) | 288
|
| Smoking ever, n (%) | 1,752 (56.9%) | 639 (61.4%) | 461 (65.9%) | 597 (56.3%) | 1,328 (56.6%) | 1,485 (56.1%) |
REFERENCES: [1] Schoevaerdts, et al. (2021). Infections in the older population: What do we know? Aging Clinical and Experimental Research, 33(3), 689–701.
[2] Strangfeld, et al. (2011). Treatment benefit or survival of the fittest: What drives the time-dependent decrease in serious infection rates under TNF inhibition? Annals of the Rheumatic Diseases, 70(11), 1914–1920.
Acknowledgments: NIL.
Disclosure of Interests: Malte Kramer: None declared, Doreen Huschek: None declared, Peter Herzer: None declared, Jacqueline Detert AbbVie, Amgen, Eli Lilly, Janssen, Galapagos, Novartis, Pfizer, UCB, Abbvie, Janssen, Johnson & Johnson, Novartis, Pfizer, Cornelia Kühne: None declared, Adrian Richter: None declared, Anja Strangfeld AbbVie, AlfaSigma, Galapagos, Janssen, Lilly, Novartis, Pfizer, Takeda and UCB, AlfaSigma, Pfizer, Joint, unconditional grant for the RABBIT register from AbbVie, Alfasigma, Biocon, BMS, Fresenius Kabi, Hexal, Lilly, Pfizer, Samsung Bioepis and Sanofi Aventis and previously from Amgen, Celltrion, MSD, Roche and UCB payed to my institution.