fetching data ... 
Objectives: To characterize systemic treatment patterns from diagnosis to last follow-up, describe transitions between therapeutic states over time, and identify baseline clinical predictors of escalation to advanced therapy with immunosuppressants and biologic agents in the largest real-world international cohort of patients with Sjögren disease.
Methods: This multinational, retrospective, observational cohort study was conducted within the Big Data Sjögren Consortium, including patients diagnosed with Sjögren disease (SjD) according to the 2002 American-European Consensus Group or 2016 ACR/EULAR classification criteria. Analysis was restricted to patients with complete information at two timepoints: baseline (at diagnosis) and cumulative follow-up (any use between diagnosis and last visit). Systemic therapies were grouped into four therapeutic lines: antimalarials, glucocorticoids, immunosuppressants, and biologic agents. From these variables, we derived a binary “ever used” variable and a four-category transition variable: never used (no use at baseline or follow-up), new start (no use at baseline, use during follow-up), discontinued (use at baseline, no use during follow-up), and continued (use at baseline with persistent or recurrent use during follow-up). Primary outcomes included: proportions of patients receiving each therapeutic line at baseline and cumulatively; treatment transitions; longitudinal therapeutic trajectories; individual drug usage patterns; and baseline predictors of immunosuppressant and/or biologic use. All tests were two-sided (p<0.05). Analyses were performed using Python 3.11 with statsmodels (v0.14) and scipy (v1.11).
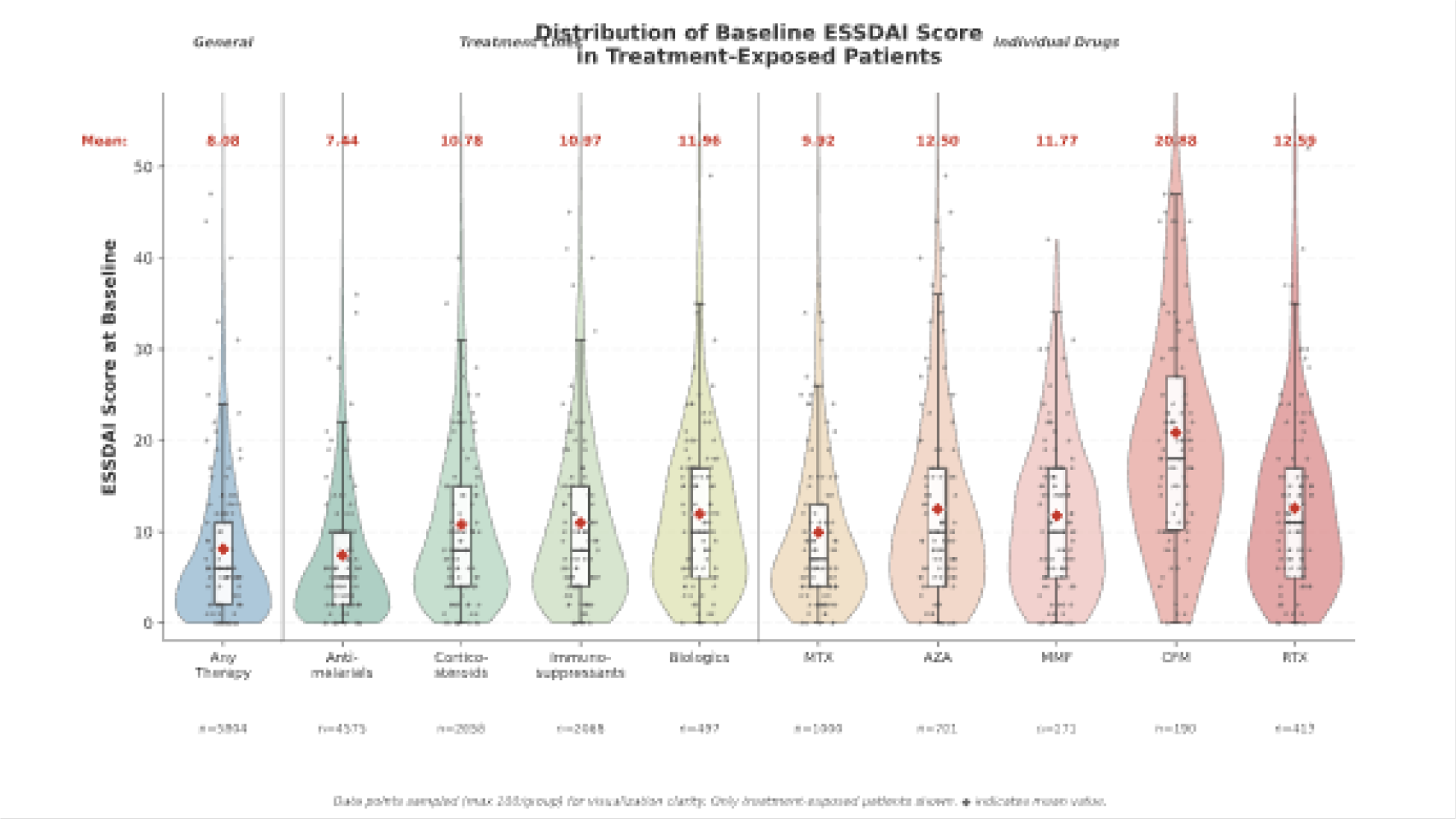
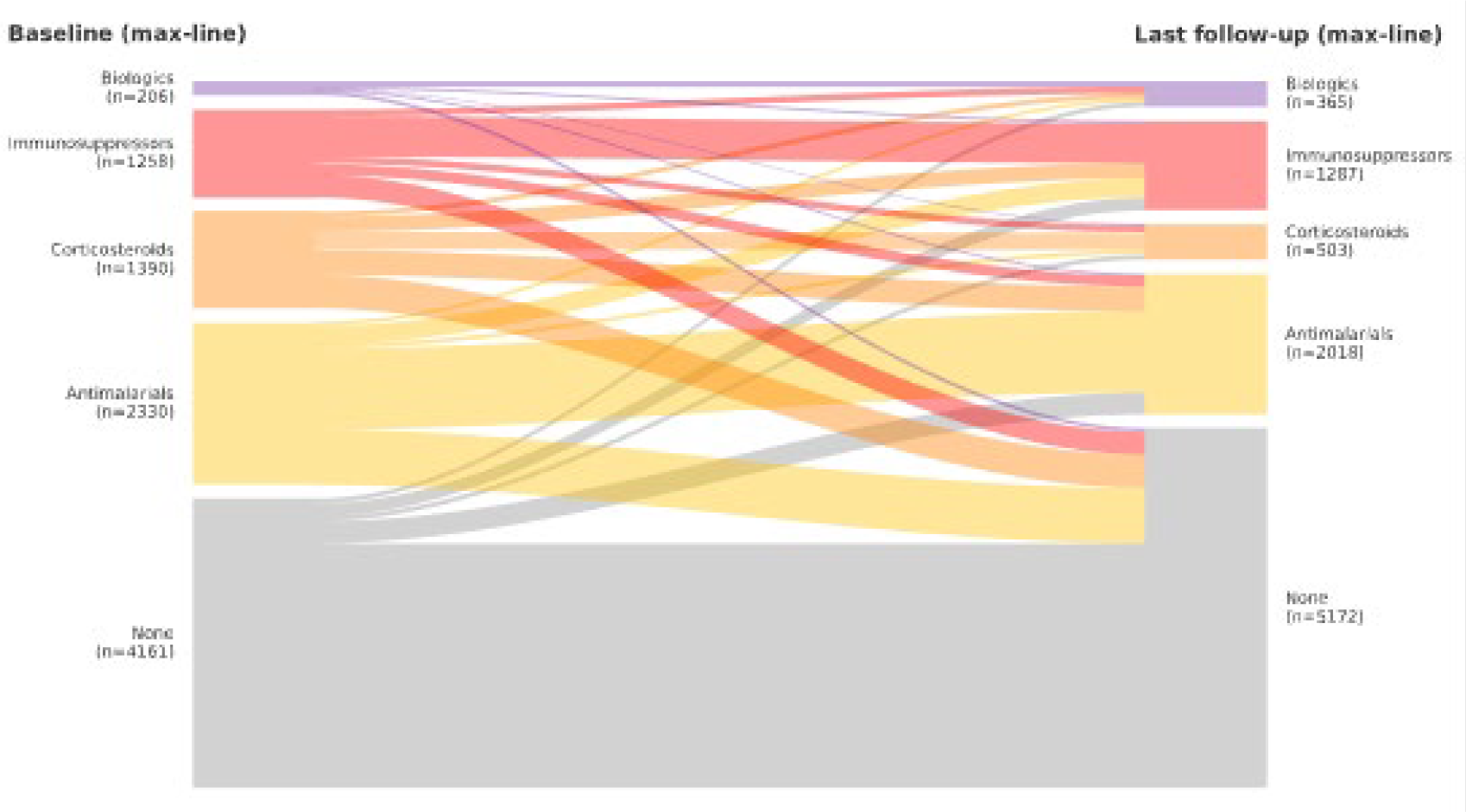
Results: Of 9,345 patients, 8,683 (92.9%) were women, with mean age at diagnosis of 51.9±14.4 years and mean follow-up of 8.3±7.5 years. Mean baseline ESSDAI score was 6.6±7.7 (median 4; IQR 2–9). According to DAS, 4,749 patients (51.3%) had low, 3,213 (34.7%) moderate, and 1,295 (14.0%) high disease activity at diagnosis. At diagnosis, 5,184 patients (55.5%) were receiving systemic therapy: antimalarials in 4,013 (42.9%), corticosteroids in 2,338 (25.0%), immunosuppressants in 1,329 (14.2%), and biologics in 206 (2.2%). Cumulatively, antimalarials were used by 4,589 patients (49.1%), corticosteroids by 2,662 (28.5%), immunosuppressants by 2,072 (22.2%), and biologics by 497 (5.3%). Individual drug exposures included methotrexate (MTX) in 1,002 (10.7%), azathioprine (AZA) in 702 (7.5%), rituximab (RTX) in 413 (4.4%), mycophenolate mofetil (MMF) in 272 (2.9%), and cyclophosphamide (CFM) in 190 (2.0%). Mean baseline ESSDAI scores increased with treatment intensity: antimalarial-exposed 7.44, corticosteroid-exposed 10.78, immunosuppressant-exposed 10.97, and biologic-exposed 11.96. For individual immunosuppressive agents, mean ESSDAI scores were: methotrexate 9.92, azathioprine 12.50, mycophenolate mofetil 11.77, rituximab 12.59, and cyclophosphamide 20.88 ( Figure 1 ). Among 7,881 patients not receiving immunosuppressants or biologics at baseline, 866 (11.0%) escalated to advanced therapy during follow-up: 725 (9.2%) initiated immunosuppressants and 193 (2.4%) initiated biologics. Among 2,072 patients who ever received immunosuppressants, 239 (11.5%) also received biologic therapy. Treatment lines increased in 1,590 patients (17.0%): 1,291 (13.8%) added one line, 255 (2.7%) two lines, and 44 (0.5%) three or more; the remaining 7,755 (83.0%) maintained the same number of lines throughout follow-up. Among 1,859 immunosuppressant users, 1,581 (85.0%) received only one agent; sequential or concomitant use of two agents occurred in 250 patients (13.4%), three agents in 27 (1.5%), and four agents in 1 (0.1%). The most common single-agent exposure was MTX (n=836; 45.0%), followed by AZA (n=494; 26.6%), MMF (n=174; 9.4%), and CFM (n=77; 4.1%). Among immunosuppressant users, 174 (9.4%) also received RTX during follow-up ( Figure 2 ). In multivariable analyses, younger age and higher disease activity were the principal predictors of advanced therapy. Each additional year of age at diagnosis was associated with 1% lower odds of immunosuppressant use (OR 0.99; 95% CI 0.99–0.99; p<0.001) and 2% lower odds of biologic use (OR 0.98; 95% CI 0.97–0.98; p<0.001). DAS was the strongest predictor: compared with low activity, moderate activity increased odds of immunosuppressant use (OR 1.47; 95% CI 1.27–1.70) and biologic use (OR 2.57; 95% CI 1.99–3.33), while high activity showed even greater associations (immunosuppressants: OR 1.71; biologics: OR 5.37; all p<0.001). For the combined outcome of immunosuppressant and/or biologic use, significant predictors included younger age (OR 0.99; 95% CI 0.98–0.99), ESSDAI score (OR 1.08 per point; 95% CI 1.06–1.09), moderate DAS (OR 1.48; 95% CI 1.28–1.71), and high DAS (OR 1.75; 95% CI 1.30–2.37; all p<0.001). The model demonstrated adequate fit (pseudo-R 2 =0.101; AIC=9,401).
Conclusions: In this multinational cohort of 9,345 patients with Sjögren disease, systemic treatment patterns were heterogeneous and followed a stepwise escalation strategy strongly influenced by disease activity and age at diagnosis. Approximately half of patients received antimalarials, one-quarter to one-third received corticosteroids or immunosuppressants, and only a minority received biologics. ESSDAI score distribution exhibited a characteristic right-skewed pattern across treatment categories, with a tail extending toward higher values among patients exposed to cyclophosphamide and rituximab. These findings provide comprehensive insights into real-world therapeutic trajectories and underscore the central role of disease activity assessment in guiding escalation to advanced systemic therapies.
Distribution of systemic disease activity according to treatment exposure status
Analysis of treatment dynamics revealed distinct patterns across therapeutic lines
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Alejandra Flores-Chávez The study was designed and developed by the Sjögren Big Data Consortium and received funds by Novartis as independent third-party sponsored investigator-initiated study. The support by Novartis was strictly limited to the provision of funds for financing the technical development of the study., Ildiko Fanny Horváth: None declared, Chiara Baldini: None declared, Roberta Priori: None declared, Arjan Vissink: None declared, Berkan Armagan: None declared, Luca Quartuccio: None declared, Gabriela Hernandez-Molina: None declared, Roberto Pereira da Costa: None declared, Agata Sebastian: None declared, Nevsun Inanc: None declared, Elena Bartoloni: None declared, Maureen Rischmueller: None declared, Fabiola Reis de Oliveira: None declared, Sandra Pasoto: None declared, Isabel Sanchez-Berna: None declared, Francesco Carubbi: None declared, Virginia Fernandes Moça Trevisani: None declared, Sheila Melchor Díaz: None declared, BRENDA MAURE NOIA: None declared, Eva Maria Fonseca-Aizpuru: None declared, Hideki Nakamura: None declared, LOPEZ DUPLA MIGUEL: None declared, Marcos Vázquez: None declared, Miriam Akasbi Montalvo: None declared, Guillem Policarpo Torres: None declared, Yasunori Suzuki: None declared, Borja De Miguel-Campo: None declared, Cecilia Fugmann: None declared, Sonja Praprotnik: None declared, Tamer A Gheita: None declared, Norma Nardi: None declared, Antónia Szántó: None declared, Emanuele Giovanni Grilli: None declared, Hendrika Bootsma: None declared, Valeria Manfrè: None declared, Levent Kiliç: None declared, Krzysztof Proc: None declared, Matilde Bandeira: None declared, Aida Shikhaliyeva: None declared, Roberto Gerli: None declared, Chandra Kirana: None declared, Manuel Ramos-Casals The study was designed and developed by the Sjögren Big Data Consortium and received funds by Novartis as independent third-party sponsored investigator-initiated study. The support by Novartis was strictly limited to the provision of funds for financing the technical development of the study., Pilar Brito-Zerón The study was designed and developed by the Sjögren Big Data Consortium and received funds by Novartis as independent third-party sponsored investigator-initiated study. The support by Novartis was strictly limited to the provision of funds for financing the technical development of the study.