fetching data ... 
Background: Physical activity is a cornerstone of spondyloarthritis (SpA) management, yet many patients limit movement due to fear of pain and negative beliefs about exercise [1]. Pain perception involves both sensory and emotional components, and the emotional dimension may foster fear-avoidance behaviours that, according to established models, sustain a self-perpetuating cycle of reduced activity, symptom persistence, and disability [2]. The differences on how fear-avoidance beliefs relate to disease activity, pain catastrophizing (PC), and quality of life between axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) have to be better understood.
Objectives: To investigate the determinants of physical activity avoidance in axSpA and PsA, and to identify clinical, demographic, and psychological factors associated with fear-avoidance beliefs.
Methods: In this monocentric observational study, 159 consecutive patients (70 axSpA, 89 PsA) attending the Rheumatology Unit of Campus Bio-Medico University Hospital (April 2023–October 2024) were enrolled. Classification criteria (ASAS 2009, CASPAR) were fulfilled; patients with fibromyalgia or major psychiatric disorders were excluded. Physical activity avoidance was assessed using the Fear-Avoidance Beliefs Questionnaire, Physical Activity subscale (FABQ-PA), defining scores ≥15 as high avoidance. Disease activity (BASDAI, DAPSA), health-related quality of life (SF-36, and its components PhCS and MCS), PC (PCS and its domains rumination, magnification, helplessness), anxiety and depression (HADS), were recorded. Group comparisons, Spearman correlations, and uni-/multivariable logistic regression models (adjusted for age, sex, BMI and disease activity indices) were performed separately for axSpA and PsA.
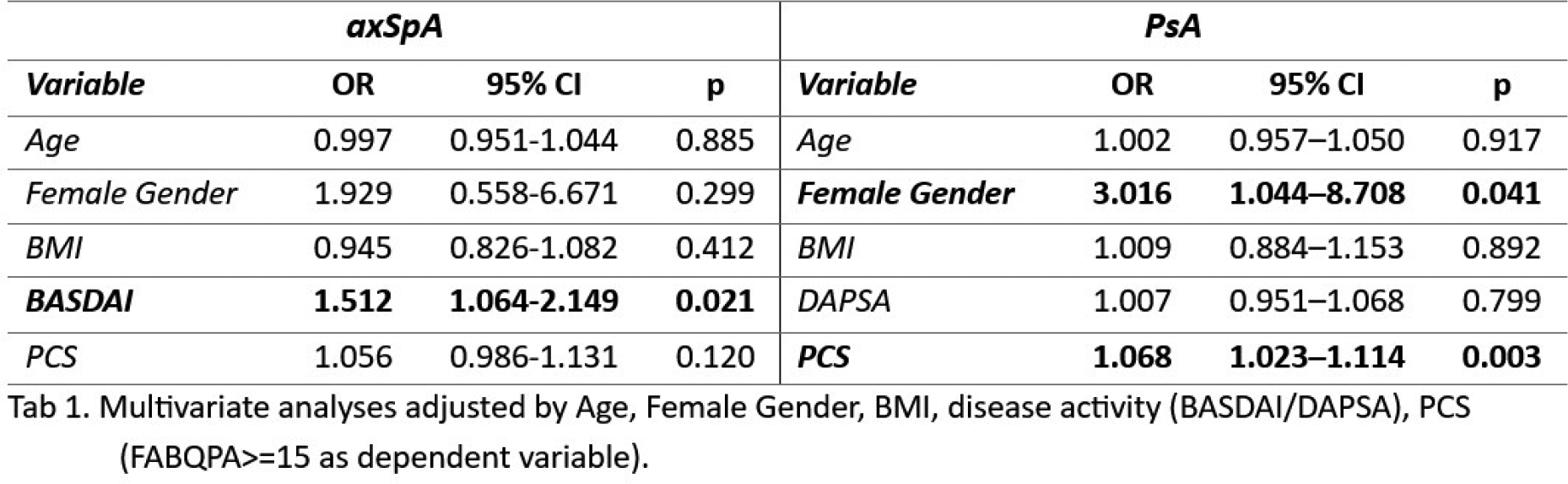
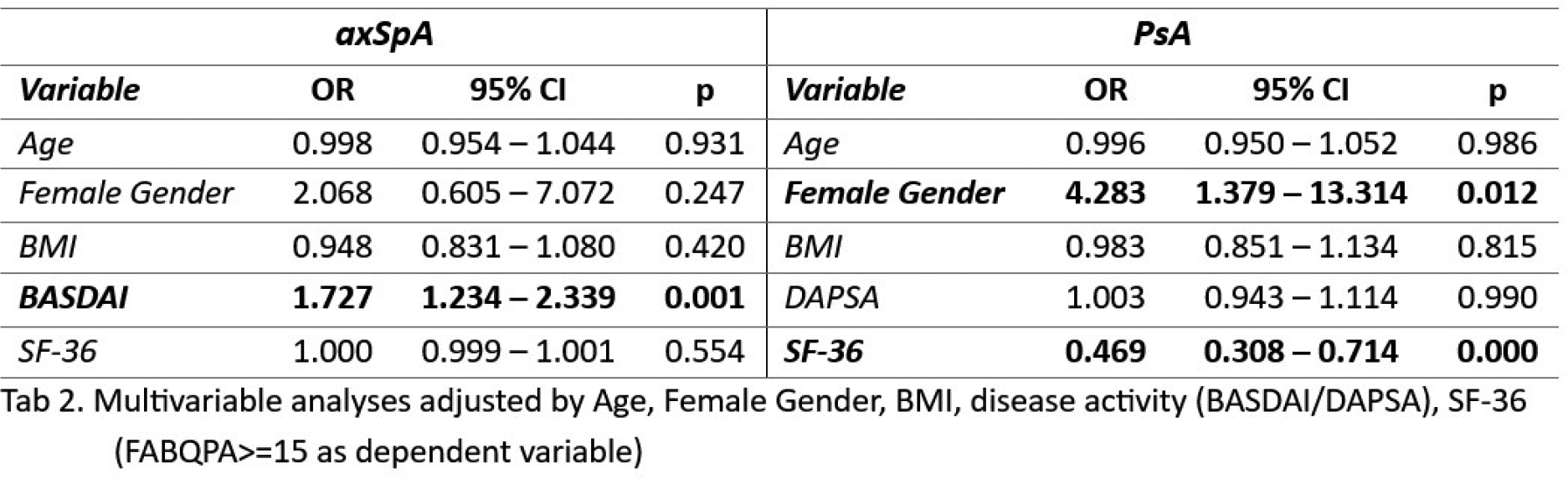
Results: High physical activity avoidance was observed in 31.4% of the cohort (32.9% axSpA, 30.3% PsA). In axSpA, patients with high avoidance showed significantly higher disease activity (BASDAI 5.5 vs 3.8, p<0.001), higher PC (25 vs 17, p=0.003) and all its domains: helplessness (11 vs 7, p<0.001), rumination (9 vs 6, p=0.007), and magnification (6 vs 5, p=0.014). Quality of life was impaired, with lower SF-36 scores (3.96 vs 5.32, p=0.008) and a trend toward lower PhCS (p=0.055) and MCS (p=0.052), while HADS-A and HADS-D did not differ. In multivariable models adjusted for age, sex, BMI, BASDAI, and including either PCS or SF-36 (Tables 1 and 2), BASDAI remained the main independent predictor of high physical activity avoidance. In additional alternative models, in which PCS or SF-36 total scores were replaced by their respective domains or components, only the PCS magnification domain retained an independent association with physical activity avoidance (OR 1.278, 95% CI 1.016–1.606, p=0.036). In PsA, no significant differences in disease activity indices were observed between patients with low and high levels of physical activity avoidance. In contrast, patients with high avoidance showed higher anxiety (HADS-A 9 vs 7.5, p=0.043), depression (HADS-D 9 vs 7, p=0.016), and PC (PCS 29 vs 18, p=0.004), driven by higher helplessness (12 vs 7, p=0.002) and rumination (10 vs 6.5, p=0.005), while magnification was not significantly different. Quality of life was markedly worse, with lower SF-36 (3.13 vs 4.60, p<0.001), PhCS (31.3 vs 38.3, p=0.002) and MCS (37.9 vs 45.0, p=0.024). In multivariable models adjusted for age, sex, BMI, DAPSA, and including either PCS or SF-36 (Tables 1 and 2), disease activity was not independently associated with physical activity avoidance. Models including PCS confirmed its independent association (OR 1.068, p=0.003); in alternative models replacing PCS with its domains, helplessness (OR 1.140, p=0.003) and rumination (OR 1.161, p=0.005) remained independently associated, whereas magnification did not. Similarly, SF-36 total score (OR 0.469, p<0.001) and its physical and mental components (PhCS OR 0.903, p=0.001; MCS OR 0.936, p=0.017) retained independent inverse associations with avoidance.
Conclusions: Physical activity avoidance in SpA reflects distinct but overlapping mechanisms. In axSpA, avoidance is primarily driven by inflammatory disease activity, whereas in PsA it appears predominantly shaped by psychological and quality of life factors. These findings support the need for phenotype-specific strategies combining optimal disease control with targeted interventions addressing maladaptive pain cognitions, particularly in PsA.
REFERENCES: [1] O’Dwyer T, O’Shea F, Wilson F. Physical activity in spondyloarthritis: a systematic review. Rheumatol Int. 2015 Mar;35(3):393-404. doi: 10.1007/s00296-014-3141-9. Epub 2014 Oct 10. PMID: 25300728.
[2] Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993 Feb;52(2):157-168. doi: 10.1016/0304-3959(93)90127-B. PMID: 8455963.
Acknowledgments: NIL.
Disclosure of Interests: None declared.